

Estimating malaria burden among pregnant women using data from antenatal care centres in Tanzania: a population-based study
- PMID: 31708150
- PMCID: PMC8752309
- DOI: 10.1016/S2214-109X(19)30405-X
Estimating malaria burden among pregnant women using data from antenatal care centres in Tanzania: a population-based study
Abstract
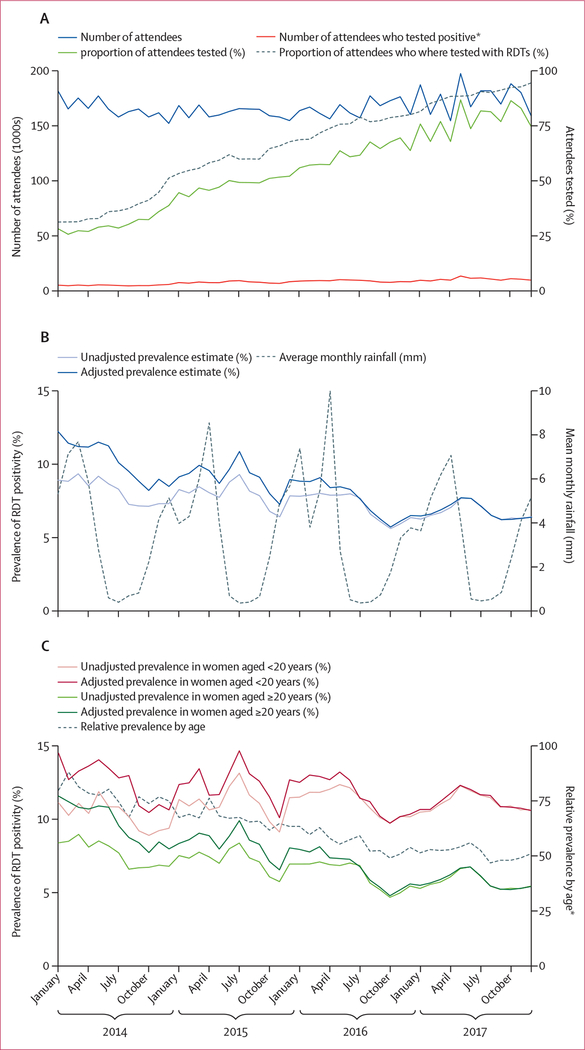
Background: More timely estimates of malaria prevalence are needed to inform optimal control strategies and measure progress. Since 2014, Tanzania has implemented nationwide malaria screening for all pregnant women within the antenatal care system. We aimed to compare malaria test results during antenatal care to two population-based prevalence surveys in Tanzanian children aged 6-59 months to examine their potential in measuring malaria trends and progress towards elimination.
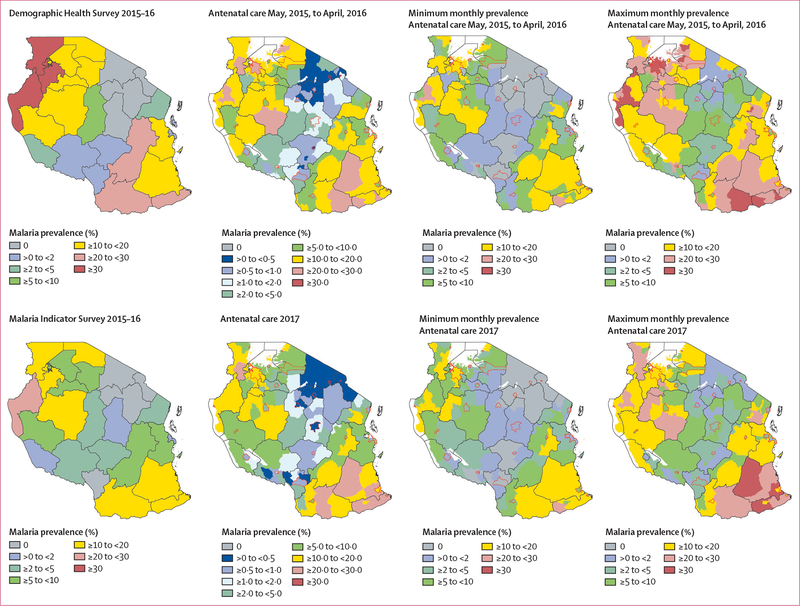
Methods: Malaria test results from pregnant women screened at their first antenatal care visits at health-care facilities (private and public) in all 184 districts of Tanzania between Jan 1, 2014, and Dec 31, 2017, were collected from the Health Management Information Systems and District Health Information System 2. We excluded facilities with no recorded antenatal care attendees during the time period. We standardised results to account for testing uptake and weighted them by the timing of two population-based surveys of childhood malaria prevalence done in 2015-16 (Demographic and Health Survey) and 2017 (Malaria Indicator Survey). We assessed regional-level correlation using Spearman's coefficient and assessed the consistency of monthly district-level prevalence ranking using Kendall's correlation coefficient.
Findings: Correlation between malaria prevalence at antenatal care and among children younger than 5 years was high (r≥0·83 for both surveys), although declines in prevalence at antenatal care were generally smaller than among children. Consistent heterogeneity (p<0·05) in antenatal care prevalence at the district level was evident in all but one region (Kilimanjaro). Data from antenatal care showed declining prevalence in three regions (Arusha, Kilimanjaro, and Manyara) where surveys estimated zero prevalence.
Interpretation: Routine antenatal care-based screening can be used to assess heterogeneity in transmission at finer resolution than population-based surveys, and provides sample sizes powered to detect changes, notably in areas of low transmission where surveys lack power. Declines in prevalence at antenatal care might lag behind those among children, highlighting the value of monitoring burden and continuing prevention efforts among pregnant women as transmission declines. The pregnancy-specific benefits and cost-effectiveness of antenatal care-based screening remain to be assessed.
Funding: None.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests
CK, DSI, EK, JRG and PW, RM, FC, SM, AM, and EJR declare no competing interests
Figures



Comment in
-
Malaria control and elimination in sub-Saharan Africa: data from antenatal care centres.Lancet Glob Health. 2019 Dec;7(12):e1595-e1596. doi: 10.1016/S2214-109X(19)30420-6. Lancet Glob Health. 2019. PMID: 31708132 No abstract available.
References
-
- WHO. Global technical strategy for malaria 2016–2030. Geneva: World Health Organization, 2015.
-
- WHO. World malaria report. Geneva: World Health Organization, 2018.
-
- WHO. Disease surveillance for malaria control: an operational manual. Geneva: World Health Organisation, 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
