

The Diagnosis and Treatment of Idiopathic Facial Paresis (Bell's Palsy)
- PMID: 31709978
- PMCID: PMC6865187
- DOI: 10.3238/arztebl.2019.0692
The Diagnosis and Treatment of Idiopathic Facial Paresis (Bell's Palsy)
Abstract
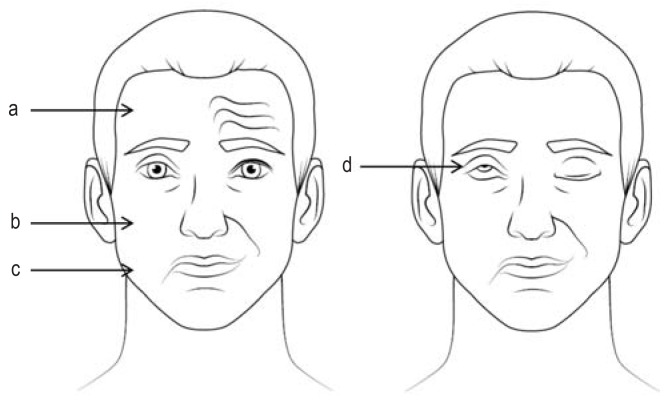
Background: Peripheral facial nerve palsy is the most com- mon functional disturbance of a cranial nerve. 60-75% of cases are idiopathic.
Methods: This review is based on a selective literature search proceeding from the current, updated German-language guideline on the diagnosis and treatment of idiopathic facial nerve palsy.
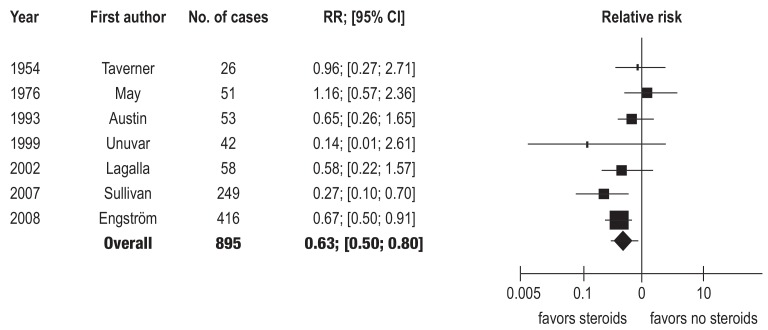
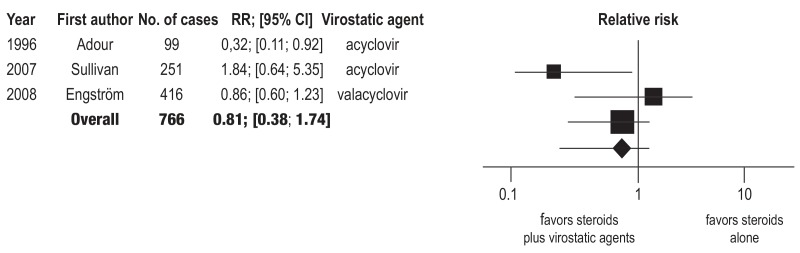
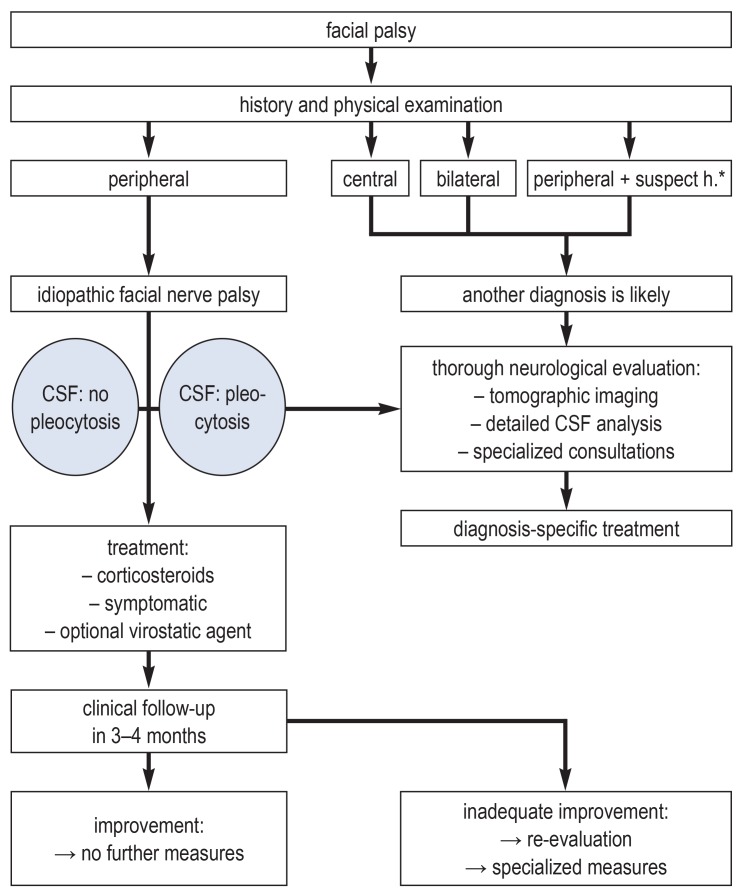
Results: The recommended drug treatment consists of prednisolone 25 mg bid for 10 days, or 60 mg qd for 5 days followed by a taper to off in decrements of 10 mg per day. This promotes full recovery (number needed to treat [NNT] = 10; 95% confidence interval [6; 20]) and lessens the risk of late sequelae such as synkinesia, autonomic disturbances, and contractures. Virostatic drugs are optional in severe cases (intense pain or suspicion of herpes zoster sine herpete) and mandatory in cases of varicella-zoster virus (VZV) infection. Corneal protection with dexpanthenol ophthalmic ointment, artificial tears, and a nocturnal moisture- retaining eye shield has been found useful in practice. In cases of incomplete recovery with residual facial weakness, both static and microsurgical dynamic methods can be used to restore facial nerve function.
Conclusion: Because 25-40% of cases of facial nerve palsy are not idiopathic, differential diagnosis is very important; key diagnostic methods include a clinical neurological examin- ation, otoscopy, and a lumbar puncture for cerebrospinal fluid examination. High-level evidence supports corticosteroid treatment for the idiopathic form of the disorder.
Figures
Comment in
-
Test Is Also Helpful in Clinically Unclear Cases of Varicella Zoster.Dtsch Arztebl Int. 2020 Mar 6;117(10):175. doi: 10.3238/arztebl.2020.0175a. Dtsch Arztebl Int. 2020. PMID: 32295697 Free PMC article. No abstract available.
-
Essential Comments.Dtsch Arztebl Int. 2020 Mar 6;117(10):175. doi: 10.3238/arztebl.2020.0175b. Dtsch Arztebl Int. 2020. PMID: 32295698 Free PMC article. No abstract available.
-
Sweet's Syndrome as Precursor of Hairy Cell Leukemia.Dtsch Arztebl Int. 2020 Mar 6;117(10):176. doi: 10.3238/arztebl.2020.0176. Dtsch Arztebl Int. 2020. PMID: 32295700 Free PMC article. No abstract available.
References
-
- Gilden DH. Bell’s palsy. N Engl J Med. 2004;351:1323–1331. - PubMed
-
- Rowlands S, Hooper R, Hughes R, Burney P. The epidemiology and treatment of Bell‘s palsy in the UK. Eur J Neurol. 2002;9:63–67. - PubMed
-
- Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell‘s palsy. N Engl J Med. 2007;357:1598–1607. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical