

1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA)
- PMID: 31709984
- PMCID: PMC8310942
- DOI: 10.1016/j.jcin.2019.11.001
1-Year Outcomes of Angina Management Guided by Invasive Coronary Function Testing (CorMicA)
Abstract
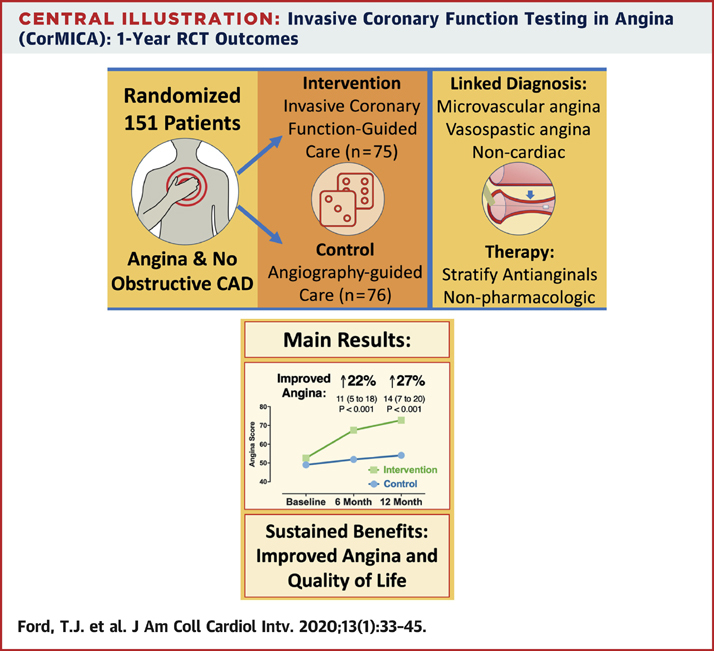
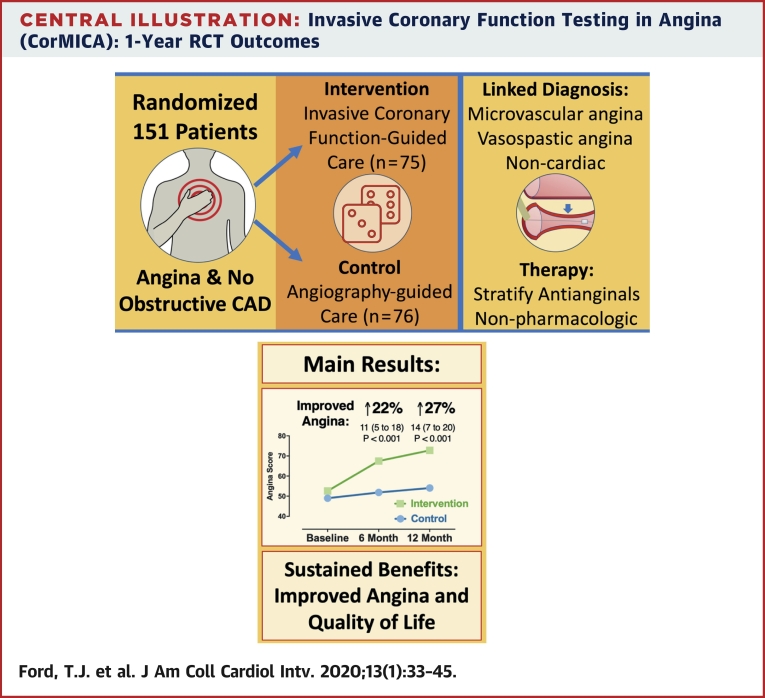
Objectives: The aim of this study was to test the hypothesis that invasive coronary function testing at time of angiography could help stratify management of angina patients without obstructive coronary artery disease.
Background: Medical therapy for angina guided by invasive coronary vascular function testing holds promise, but the longer-term effects on quality of life and clinical events are unknown among patients without obstructive disease.
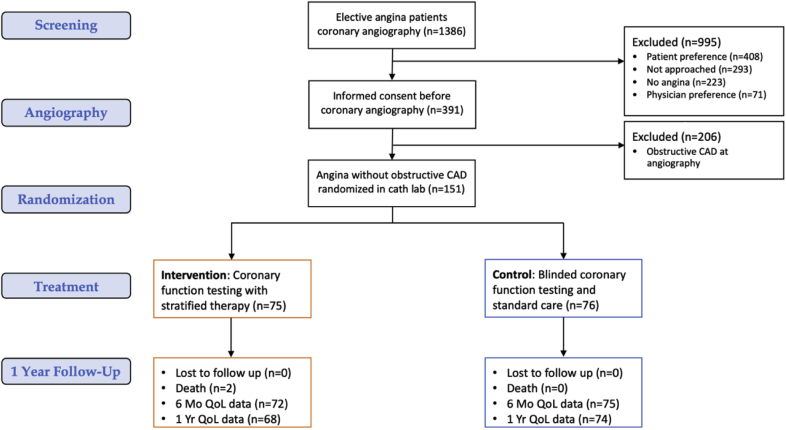
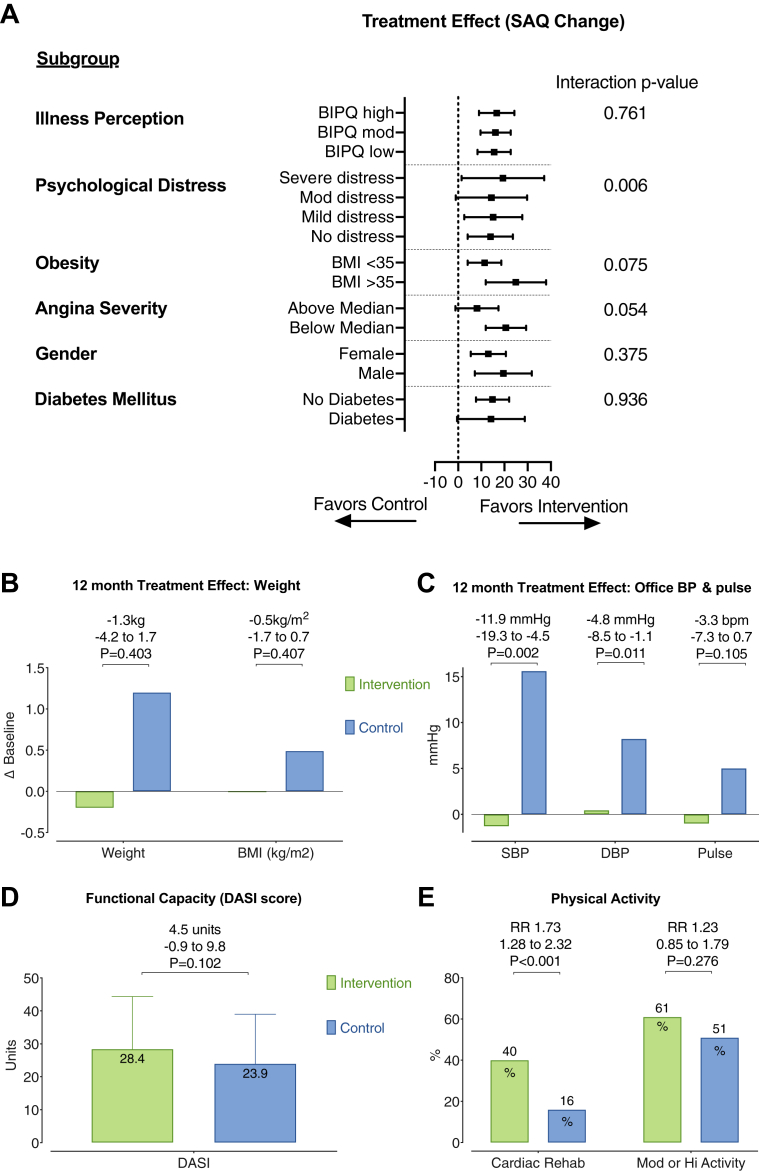
Methods: A total of 151 patients with angina with symptoms and/or signs of ischemia and no obstructive coronary artery disease were randomized to stratified medical therapy guided by an interventional diagnostic procedure versus standard care (control group with blinded interventional diagnostic procedure results). The interventional diagnostic procedure-facilitated diagnosis (microvascular angina, vasospastic angina, both, or neither) was linked to guideline-based management. Pre-specified endpoints included 1-year patient-reported outcome measures (Seattle Angina Questionnaire, quality of life [EQ-5D]) and major adverse cardiac events (all-cause mortality, myocardial infarction, unstable angina hospitalization or revascularization, heart failure hospitalization, and cerebrovascular event) at subsequent follow-up.
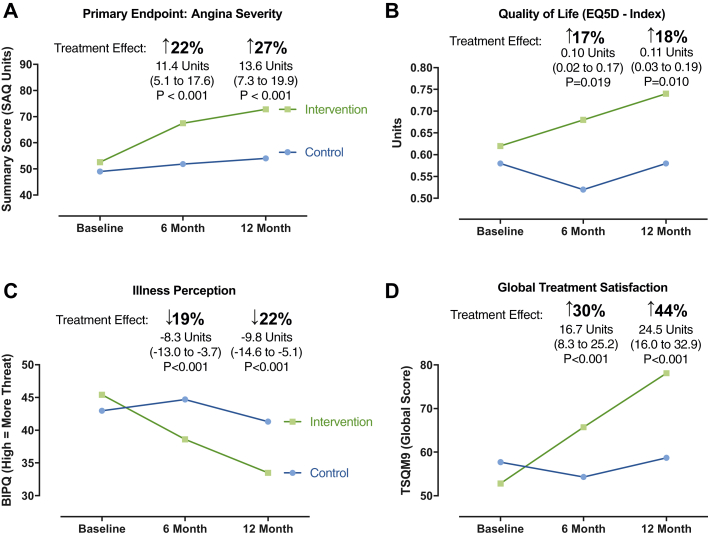
Results: Between November 2016 and December 2017, 151 patients with ischemia and no obstructive coronary artery disease were randomized (n = 75 to the intervention group, n = 76 to the control group). At 1 year, overall angina (Seattle Angina Questionnaire summary score) improved in the intervention group by 27% (difference 13.6 units; 95% confidence interval: 7.3 to 19.9; p < 0.001). Quality of life (EQ-5D index) improved in the intervention group relative to the control group (mean difference 0.11 units [18%]; 95% confidence interval: 0.03 to 0.19; p = 0.010). After a median follow-up duration of 19 months (interquartile range: 16 to 22 months), major adverse cardiac events were similar between the groups, occurring in 9 subjects (12%) in the intervention group and 8 (11%) in the control group (p = 0.803).
Conclusions: Stratified medical therapy in patients with ischemia and no obstructive coronary artery disease leads to marked and sustained angina improvement and better quality of life at 1 year following invasive coronary angiography. (Coronary Microvascular Angina [CorMicA]; NCT03193294).
Keywords: coronary physiology; elective coronary angiography; microvascular angina; stable angina pectoris; stratified medicine; vasospastic angina.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Treating Coronary Microvascular Dysfunction as the "Culprit" Lesion in Patients With Refractory Angina: Lessons From CorMicA at 1 Year.JACC Cardiovasc Interv. 2020 Jan 13;13(1):46-48. doi: 10.1016/j.jcin.2019.12.001. JACC Cardiovasc Interv. 2020. PMID: 31918941 No abstract available.
References
-
- Tavella R., Cutri N., Tucker G., Adams R., Spertus J., Beltrame J.F. Natural history of patients with insignificant coronary artery disease. Eur Heart J Qual Care Clin Outcomes. 2016;2:117–124. - PubMed
-
- Jespersen L., Hvelplund A., Abildstrom S.Z. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–744. - PubMed
-
- Suda A., Takahashi J., Hao K. Coronary functional abnormalities in patients with angina and nonobstructive coronary artery disease. J Am Coll Cardiol. 2019;74:2350–2360. - PubMed
