

Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction
- PMID: 31710673
- PMCID: PMC7061278
- DOI: 10.1093/cvr/cvz301
Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction
Abstract
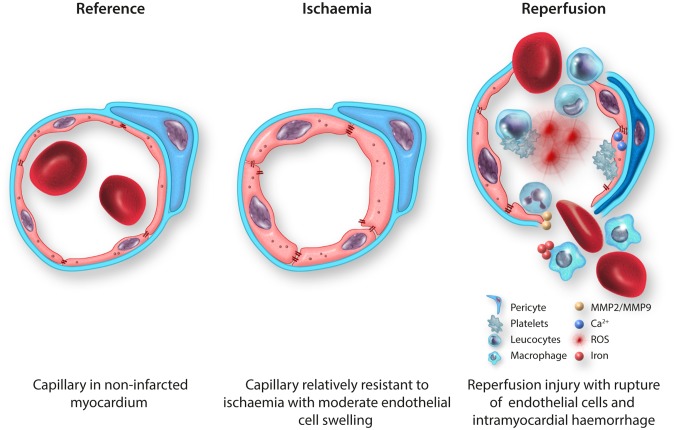
Early mechanical reperfusion of the epicardial coronary artery by primary percutaneous coronary intervention (PCI) is the guideline-recommended treatment for ST-elevation myocardial infarction (STEMI). Successful restoration of epicardial coronary blood flow can be achieved in over 95% of PCI procedures. However, despite angiographically complete epicardial coronary artery patency, in about half of the patients perfusion to the distal coronary microvasculature is not fully restored, which is associated with increased morbidity and mortality. The exact pathophysiological mechanism of post-ischaemic coronary microvascular dysfunction (CMD) is still debated. Therefore, the current review discusses invasive and non-invasive techniques for the diagnosis and quantification of CMD in STEMI in the clinical setting as well as results from experimental in vitro and in vivo models focusing on ischaemic-, reperfusion-, and inflammatory damage to the coronary microvascular endothelial cells. Finally, we discuss future opportunities to prevent or treat CMD in STEMI patients.
Keywords: Coronary microvascular dysfunction; Coronary microvascular endothelial cells; Intramyocardial haemorrhage; Microvascular reperfusion injury; ST-elevation myocardial infarction.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Cohen M, Boiangiu C, Abidi M.. Therapy for ST-segment elevation myocardial infarction patients who present late or are ineligible for reperfusion therapy. J Am Coll Cardiol 2010;55:1895–1906. - PubMed
-
- Van Kranenburg MV, Magro M, Thiele H, DeWaha S, Eitel I, Cochet A, Cottin Y, Atar D, Buser P, Wu E, Lee D, Bodi V, Klug G, Metzler B, Delewi R, Bernhardt P, Rottbauer W, Boersma E, Zijlstra F, Geuns RJ.. Prognostic value of microvascular obstruction and infarct size, as measured by CMR in STEMI patients. JACC Cardiovasc Imaging 2014;7:930–939. - PubMed
-
- Reffelmann T, Kloner RA.. Microvascular reperfusion injury: rapid expansion of anatomic no reflow during reperfusion in the rabbit. Am J Physiol Circ Physiol 2002;283:H1099–H1107. - PubMed
-
- Lima JAC, Wu KC, Becker LC, Melin JA, Gerber BL, Rochitte CE, Bluemke DA, McVeigh ER.. Microvascular obstruction and left ventricular remodeling early after acute myocardial infarction. Circulation 2012;101:2734–2741. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
