

The Predictive Approaches to Treatment effect Heterogeneity (PATH) Statement
- PMID: 31711134
- PMCID: PMC7531587
- DOI: 10.7326/M18-3667
The Predictive Approaches to Treatment effect Heterogeneity (PATH) Statement
Abstract
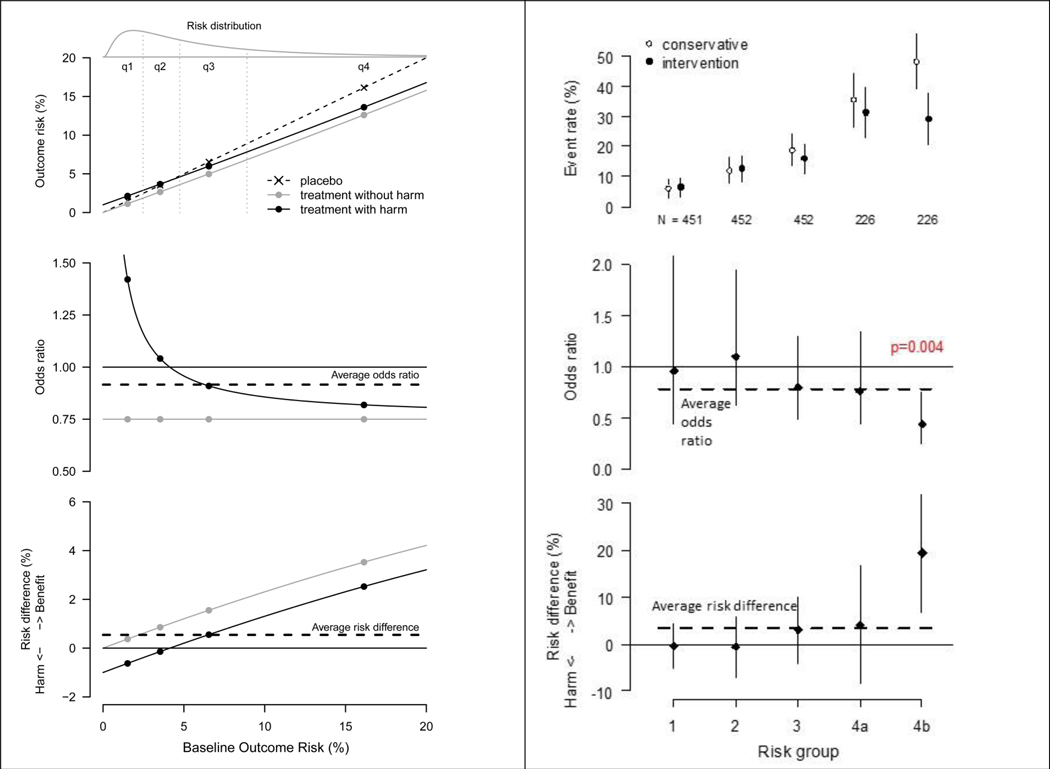
Heterogeneity of treatment effect (HTE) refers to the nonrandom variation in the magnitude or direction of a treatment effect across levels of a covariate, as measured on a selected scale, against a clinical outcome. In randomized controlled trials (RCTs), HTE is typically examined through a subgroup analysis that contrasts effects in groups of patients defined "1 variable at a time" (for example, male vs. female or old vs. young). The authors of this statement present guidance on an alternative approach to HTE analysis, "predictive HTE analysis." The goal of predictive HTE analysis is to provide patient-centered estimates of outcome risks with versus without the intervention, taking into account all relevant patient attributes simultaneously. The PATH (Predictive Approaches to Treatment effect Heterogeneity) Statement was developed using a multidisciplinary technical expert panel, targeted literature reviews, simulations to characterize potential problems with predictive approaches, and a deliberative process engaging the expert panel. The authors distinguish 2 categories of predictive HTE approaches: a "risk-modeling" approach, wherein a multivariable model predicts the risk for an outcome and is applied to disaggregate patients within RCTs to define risk-based variation in benefit, and an "effect-modeling" approach, wherein a model is developed on RCT data by incorporating a term for treatment assignment and interactions between treatment and baseline covariates. Both approaches can be used to predict differential absolute treatment effects, the most relevant scale for clinical decision making. The authors developed 4 sets of guidance: criteria to determine when risk-modeling approaches are likely to identify clinically important HTE, methodological aspects of risk-modeling methods, considerations for translation to clinical practice, and considerations and caveats in the use of effect-modeling approaches. The PATH Statement, together with its explanation and elaboration document, may guide future analyses and reporting of RCTs.
Figures
Comment in
-
Advancing Personalized Medicine Through Prediction.Ann Intern Med. 2020 Jan 7;172(1):63-64. doi: 10.7326/M19-3010. Epub 2019 Nov 12. Ann Intern Med. 2020. PMID: 31711098 No abstract available.
-
The Predictive Approaches to Treatment effect Heterogeneity (PATH) Statement.Ann Intern Med. 2020 Jun 2;172(11):776. doi: 10.7326/L20-0427. Ann Intern Med. 2020. PMID: 32479147 No abstract available.
-
The Predictive Approaches to Treatment effect Heterogeneity (PATH) Statement.Ann Intern Med. 2020 Jun 2;172(11):775-776. doi: 10.7326/L20-0426. Ann Intern Med. 2020. PMID: 32479148 No abstract available.
References
-
- Rothwell PM. Can overall results of clinical trials be applied to all patients? Lancet 1995; 345(8965):1616–1619. - PubMed
-
- Rothwell PM, Mehta Z, Howard SC, Gutnikov SA, Warlow CP. Treating individuals 3: from subgroups to individuals: general principles and the example of carotid endarterectomy. Lancet 2005; 365(9455):256–265. - PubMed
-
- Kent DM, Hayward RA. Limitations of applying summary results of clinical trials to individual patients: the need for risk stratification. JAMA 2007; 298(10):1209–1212. - PubMed
-
- Hayward RA, Kent DM, Vijan S, Hofer TP. Reporting clinical trial results to inform providers, payers, and consumers. Health Aff (Millwood ) 2005; 24(6):1571–1581. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources