

Circulating Tumor DNA Analysis for Detection of Minimal Residual Disease After Chemoradiotherapy for Localized Esophageal Cancer
- PMID: 31711920
- PMCID: PMC7010551
- DOI: 10.1053/j.gastro.2019.10.039
Circulating Tumor DNA Analysis for Detection of Minimal Residual Disease After Chemoradiotherapy for Localized Esophageal Cancer
Abstract
Background & aims: Biomarkers are needed to risk stratify after chemoradiotherapy for localized esophageal cancer. These could improve identification of patients at risk for cancer progression and selection of additional therapy.
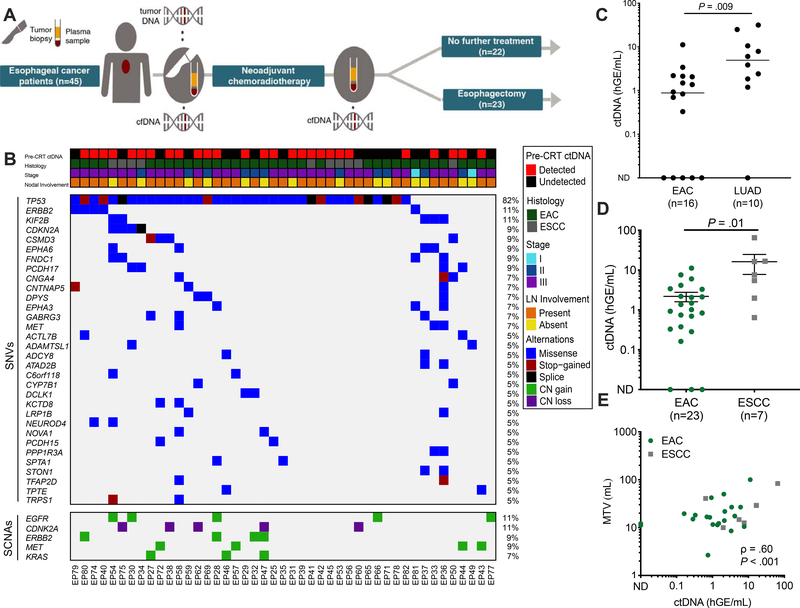
Methods: We performed deep sequencing (CAncer Personalized Profiling by deep Sequencing, [CAPP-Seq]) analyses of plasma cell-free DNA collected from 45 patients before and after chemoradiotherapy for esophageal cancer, as well as DNA from leukocytes and fixed esophageal tumor biopsy samples collected during esophagogastroduodenoscopy. Patients were treated from May 2010 through October 2015; 23 patients subsequently underwent esophagectomy, and 22 did not undergo surgery. We also sequenced DNA from blood samples from 40 healthy control individuals. We analyzed 802 regions of 607 genes for single-nucleotide variants previously associated with esophageal adenocarcinoma or squamous cell carcinoma. Patients underwent imaging analyses 6-8 weeks after chemoradiotherapy and were followed for 5 years. Our primary aim was to determine whether detection of circulating tumor DNA (ctDNA) after chemoradiotherapy is associated with risk of tumor progression (growth of local, regional, or distant tumors, detected by imaging or biopsy).
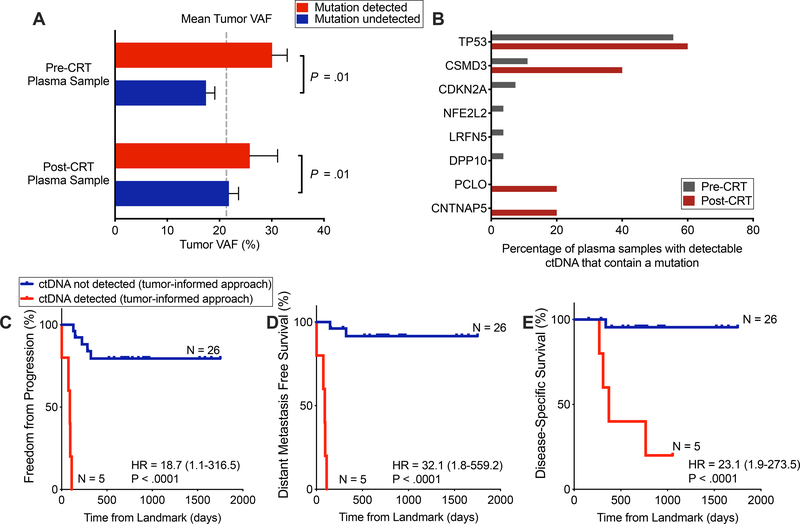
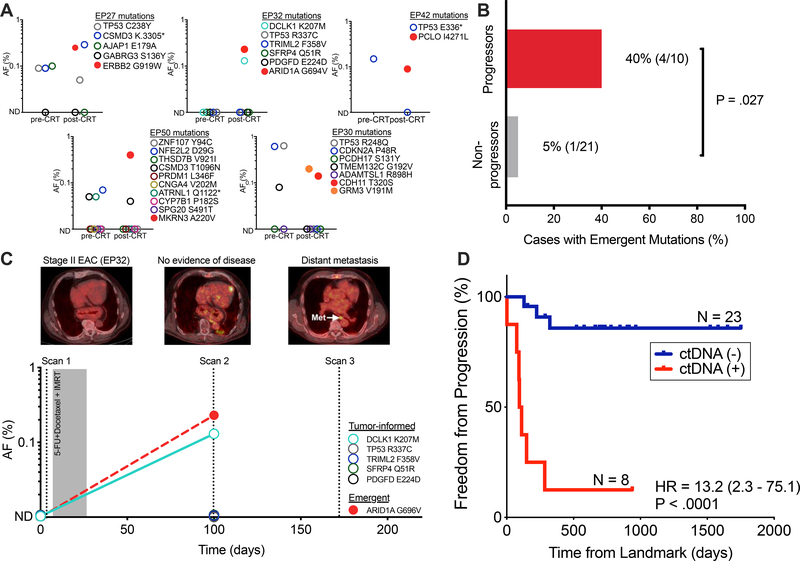
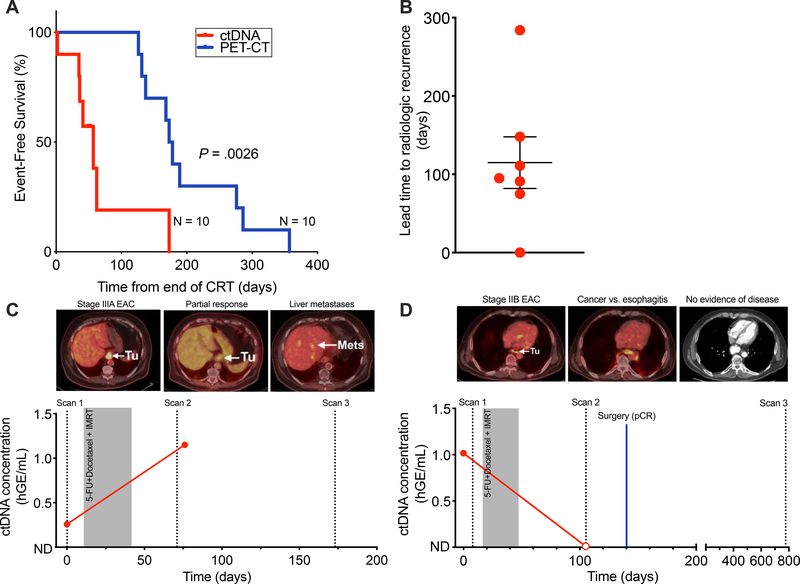
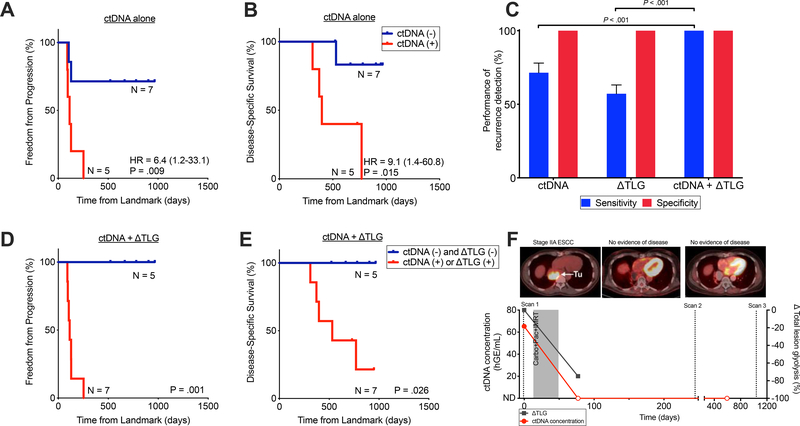
Results: The median proportion of tumor-derived DNA in total cell-free DNA before treatment was 0.07%, indicating that ultrasensitive assays are needed for quantification and analysis of ctDNA from localized esophageal tumors. Detection of ctDNA after chemoradiotherapy was associated with tumor progression (hazard ratio, 18.7; P < .0001), formation of distant metastases (hazard ratio, 32.1; P < .0001), and shorter disease-specific survival times (hazard ratio, 23.1; P < .0001). A higher proportion of patients with tumor progression had new mutations detected in plasma samples collected after chemoradiotherapy than patients without progression (P = .03). Detection of ctDNA after chemoradiotherapy preceded radiographic evidence of tumor progression by an average of 2.8 months. Among patients who received chemoradiotherapy without surgery, combined ctDNA and metabolic imaging analysis predicted progression in 100% of patients with tumor progression, compared with 71% for only ctDNA detection and 57% for only metabolic imaging analysis (P < .001 for comparison of either technique to combined analysis).
Conclusions: In an analysis of cell-free DNA in blood samples from patients who underwent chemoradiotherapy for esophageal cancer, detection of ctDNA was associated with tumor progression, metastasis, and disease-specific survival. Analysis of ctDNA might be used to identify patients at highest risk for tumor progression.
Keywords: Chemoradiotherapy; Genetics; Polymorphism; SNP.
Copyright © 2020 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med 2012;366:2074–84. - PubMed
-
- Shapiro J, van Lanschot JJB, Hulshof M, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol 2015;16:1090–1098. - PubMed
-
- Noordman BJ, Spaander MCW, Valkema R, et al. Detection of residual disease after neoadjuvant chemoradiotherapy for oesophageal cancer (preSANO): a prospective multicentre, diagnostic cohort study. Lancet Oncol 2018. - PubMed
-
- Bedenne L, Michel P, Bouche O, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol 2007;25:1160–8. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
