

Cancer-associated retinopathy in ampullary pancreatic cancer
- PMID: 31712238
- PMCID: PMC6855908
- DOI: 10.1136/bcr-2019-231444
Cancer-associated retinopathy in ampullary pancreatic cancer
Abstract
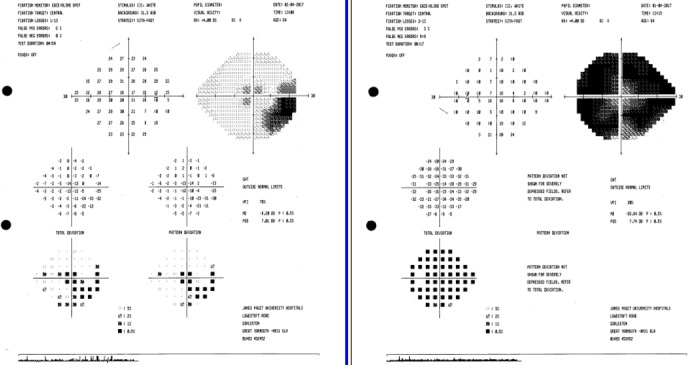
A 64-year-old woman presented with bilateral visual loss with shimmering photopsias as the only clinical manifestation of an occult pancreatic ampullary adenocarcinoma causing duct dilatation. Abnormal electroretinograms led to suspicion of cancer-associated retinopathy (CAR), and CT of the abdomen showed an underlying pancreatic malignancy, detected with subclinical liver function tests following diagnosis of CAR. Biopsy showed a T2N0M0 ampullary adenocarcinoma. The patient was managed with Whipple's procedure and adjuvant chemotherapy and has made a good recovery with no progression of her retinopathy. To our knowledge, this is one of the first descriptions of CAR in the context of pancreatic malignancy. It is atypical in its asymmetric presentation and favourable patient outcome. CAR is an important diagnosis to make, as ocular manifestations can be the only indication of an occult malignancy, resulting in a swifter diagnosis and potentially life-saving early intervention.
Keywords: ophthalmology; pancreatic cancer; retina.
© BMJ Publishing Group Limited 2019. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical