

Twenty-Four Hour Urine Testing and Prescriptions for Urinary Stone Disease-Related Medications in Veterans
- PMID: 31712387
- PMCID: PMC6895498
- DOI: 10.2215/CJN.03580319
Twenty-Four Hour Urine Testing and Prescriptions for Urinary Stone Disease-Related Medications in Veterans
Abstract
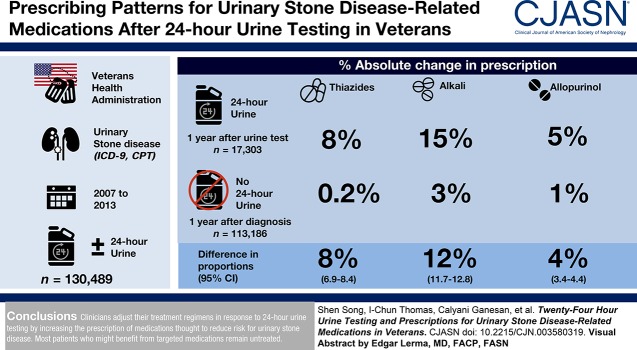
Background and objectives: Current guidelines recommend 24-hour urine testing in the evaluation and treatment of persons with high-risk urinary stone disease. However, how much clinicians use information from 24-hour urine testing to guide secondary prevention strategies is unknown. We sought to determine the degree to which clinicians initiate or continue stone disease-related medications in response to 24-hour urine testing.
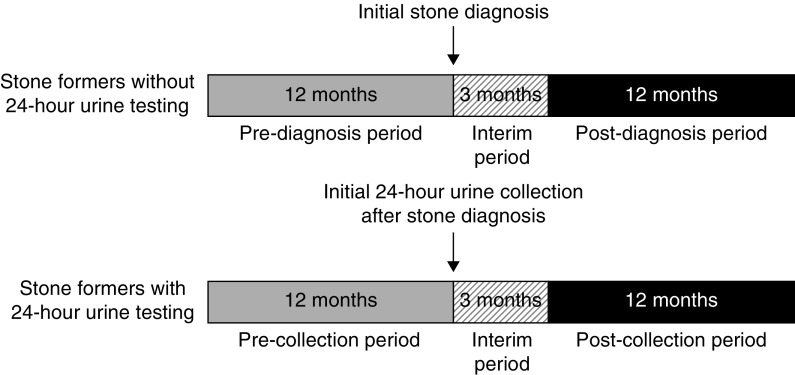
Design, setting, participants, & measurements: We examined a national cohort of 130,489 patients with incident urinary stone disease in the Veterans Health Administration between 2007 and 2013 to determine whether prescription patterns for thiazide diuretics, alkali therapy, and allopurinol changed in response to 24-hour urine testing.
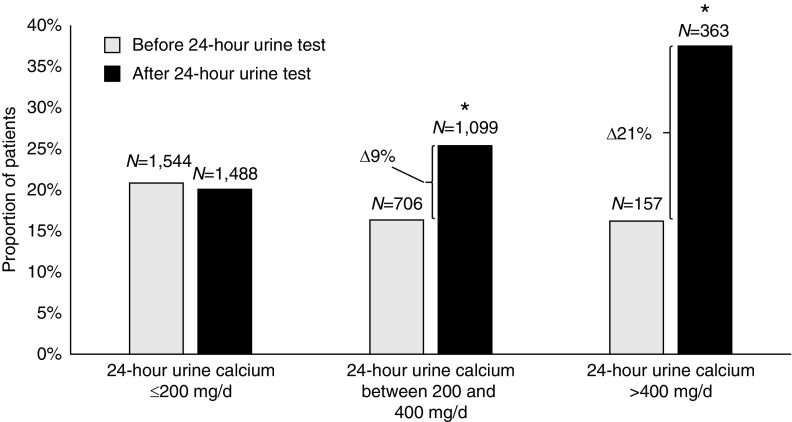
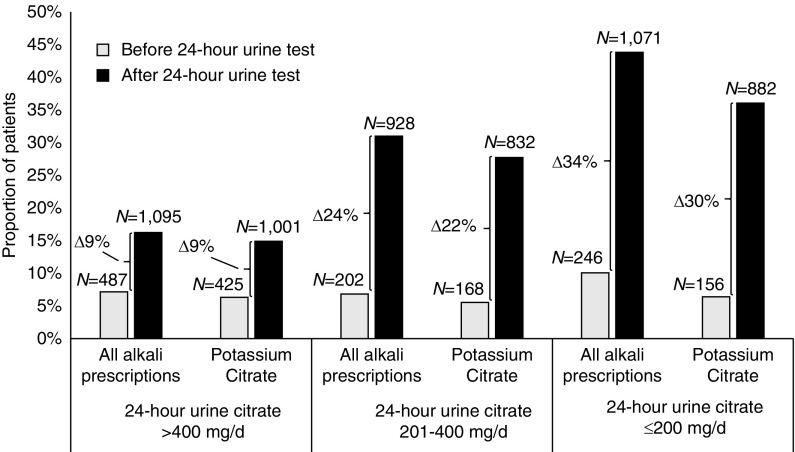
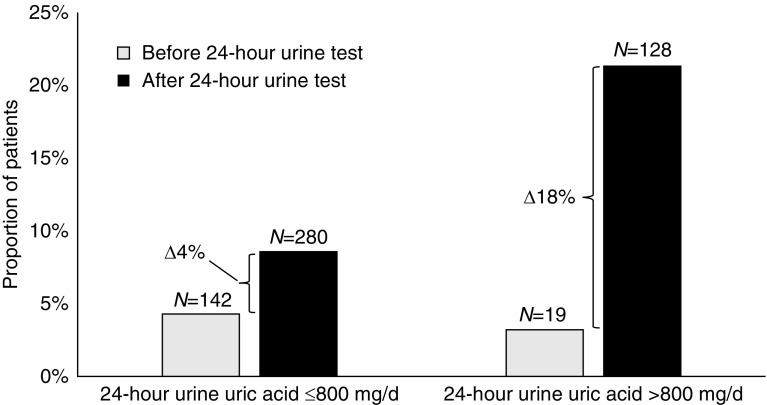
Results: Stone formers who completed 24-hour urine testing (n=17,303; 13%) were significantly more likely to be prescribed thiazide diuretics, alkali therapy, and allopurinol compared with those who did not complete a 24-hour urine test (n=113,186; 87%). Prescription of thiazide diuretics increased in patients with hypercalciuria (9% absolute increase if urine calcium 201-400 mg/d; 21% absolute increase if urine calcium >400 mg/d, P<0.001). Prescription of alkali therapy increased in patients with hypocitraturia (24% absolute increase if urine citrate 201-400 mg/d; 34% absolute increase if urine citrate ≤200 mg/d, P<0.001). Prescription of allopurinol increased in patients with hyperuricosuria (18% absolute increase if urine uric acid >800 mg/d, P<0.001). Patients who had visited both a urologist and a nephrologist within 6 months of 24-hour urine testing were more likely to have been prescribed stone-related medications than patients who visited one, the other, or neither.
Conclusions: Clinicians adjust their treatment regimens in response to 24-hour urine testing by increasing the prescription of medications thought to reduce risk for urinary stone disease. Most patients who might benefit from targeted medications remain untreated.
Keywords: 24-hour urine; United States Department of Veterans Affairs; Veterans Health Administration; alkalies; allopurinol; calcium; citrates; citric acid; cohort studies; humans; hypercalciuria; kidney stones; medications; nephrologists; secondary prevention; sodium chloride symporter inhibitors; thiazides; uric acid; urinary calculi; urinary stone disease; urologists; veterans; veterans health.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Gaps in Care among Veterans with Urinary Stone Disease.Clin J Am Soc Nephrol. 2019 Dec 6;14(12):1690-1691. doi: 10.2215/CJN.12131019. Epub 2019 Nov 11. Clin J Am Soc Nephrol. 2019. PMID: 31811085 Free PMC article. No abstract available.
-
Re: Twenty-Four Hour Urine Testing and Prescriptions for Urinary Stone Disease-Related Medications in Veterans.J Urol. 2020 Jun;203(6):1056-1057. doi: 10.1097/JU.0000000000000997.01. Epub 2020 Mar 10. J Urol. 2020. PMID: 32155362 No abstract available.
References
-
- Stamatelou KK, Francis ME, Jones CA, Nyberg LM, Curhan GC: Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney Int 63: 1817–1823, 2003 - PubMed
-
- Sutherland JW, Parks JH, Coe FL: Recurrence after a single renal stone in a community practice. Miner Electrolyte Metab 11: 267–269, 1985 - PubMed
-
- Trinchieri A, Ostini F, Nespoli R, Rovera F, Montanari E, Zanetti G: A prospective study of recurrence rate and risk factors for recurrence after a first renal stone. J Urol 162: 27–30, 1999 - PubMed
-
- Pearle MS, Goldfarb DS, Assimos DG, Curhan G, Denu-Ciocca CJ, Matlaga BR, Monga M, Penniston KL, Preminger GM, Turk TM, White JR; American Urological Assocation : Medical management of kidney stones: AUA guideline. J Urol 192: 316–324, 2014 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
