

Range Variability in CMR Feature Tracking Multilayer Strain across Different Stages of Heart Failure
- PMID: 31712641
- PMCID: PMC6848170
- DOI: 10.1038/s41598-019-52683-8
Range Variability in CMR Feature Tracking Multilayer Strain across Different Stages of Heart Failure
Abstract
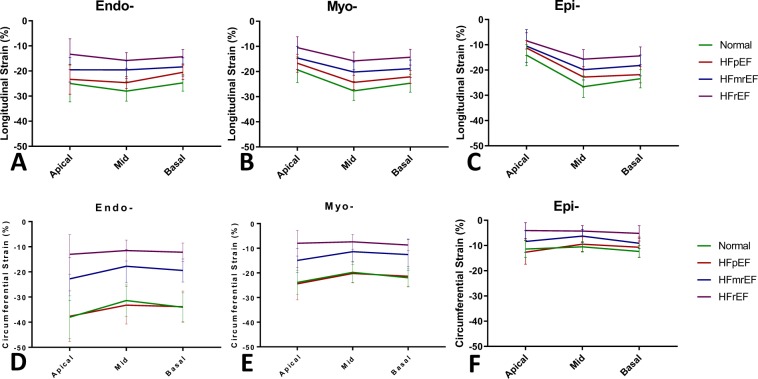
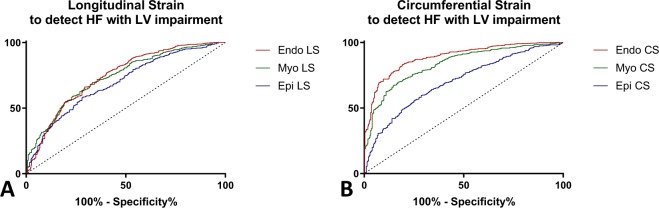
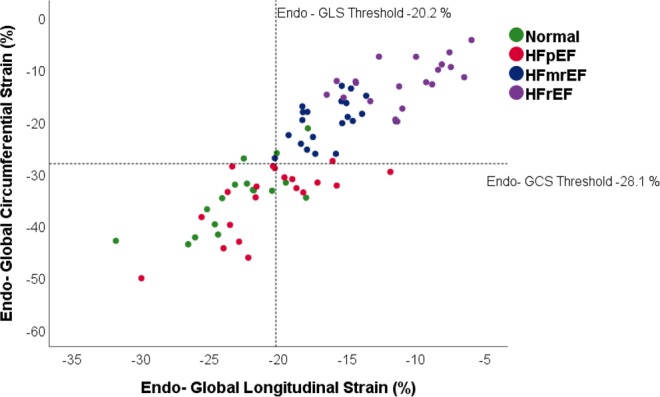
Heart failure (HF) is associated with progressive ventricular remodeling and impaired contraction that affects distinctly various regions of the myocardium. Our study applied cardiac magnetic resonance (CMR) feature tracking (FT) to assess comparatively myocardial strain at 3 distinct levels: subendocardial (Endo-), mid (Myo-) and subepicardial (Epi-) myocardium across an extended spectrum of patients with HF. 59 patients with HF, divided into 3 subgroups as follows: preserved ejection fraction (HFpEF, N = 18), HF with mid-range ejection fraction (HFmrEF, N = 21), HF with reduced ejection fraction (HFrEF, N = 20) and a group of age- gender- matched volunteers (N = 17) were included. Using CMR FT we assessed systolic longitudinal and circumferential strain and strain-rate at Endo-, Myo- and Epi- levels. Strain values were the highest in the Endo- layer and progressively lower in the Myo- and Epi- layers respectively, this gradient was present in all the patients groups analyzed but decreased progressively in HFmrEF and further on in HFrEF groups. GLS decreased with the severity of the disease in all 3 layers: Normal > HFpEF > HFmrEF > HFrEF (Endo-: -23.0 ± 3.5 > -20.0 ± 3.3 > -16.4 ± 2.2 > -11.0 ± 3.2, p < 0.001, Myo-: -20.7 ± 2.4 > -17.5.0 ± 2.6 > -14.5 ± 2.1 > -9.6 ± 2.7, p < 0.001; Epi-: -15.7 ± 1.9 > -12.2 ± 2.1 > -10.6 ± 2.3 > -7.7 ± 2.3, p < 0.001). In contrast, GCS was not different between the Normal and HFpEF (Endo-: -34.5 ± 6.2 vs -33.9 ± 5.7, p = 0.51; Myo-: -21.9 ± 3.8 vs -21.3 ± 2.2, p = 0.39, Epi-: -11.4 ± 2.0 vs -10.9 ± 2.3, p = 0.54) but was, as well, markedly lower in the systolic heart failure groups: Normal > HFmrEF > HFrEF (Endo-: -34.5 ± 6.2 > -20.0 ± 4.2 > 12.3 ± 4.2, p < 0.001; Myo-: -21.9 ± 3.8 > -13.0 ± 3.4 > -8.0 ± 2.7. p < 0.001; Epi-: -11.4 ± 2.0 > -7.9 ± 2.3 > -4.5 ± 1.9. p < 0.001). CMR feature tracking multilayer strain assessment identifies large range differences between distinct myocardial regions. Our data emphasizes the importance of sub-endocardial myocardium for cardiac contraction and thus, its predilect role in imaging detection of functional impairment. CMR feature tracking offers a convenient, readily available, platform to evaluate myocardial contraction with excellent spatial resolution, rendering further details about discrete areas of the myocardium. Using this technique across distinct groups of patients with heart failure (HF), we demonstrate that subendocardial regions of the myocardium exhibit much higher strain values than mid-myocardium or subepicardial and are more sensitive to detect contractile impairment. We also show comparatively higher values of circumferential strain compared with longitudinal and a higher sensitivity to detect contractile impairment. A newly characterized group of patients, HF with mid-range ejection fraction (EF), shows similar traits of decompensation but has relatively higher strain values as patients with HF with reduced EF.
Conflict of interest statement
The authors declare no competing interests.
Figures

 ) normal age-, gender- matched control, HFpEF (
) normal age-, gender- matched control, HFpEF ( ) patients with HF with preserved EF, HFmrEF (
) patients with HF with preserved EF, HFmrEF ( ) patients with HF with mid-range reduced EF, HFrEF (
) patients with HF with mid-range reduced EF, HFrEF ( ) patients with HF with reduced EF.
) patients with HF with reduced EF.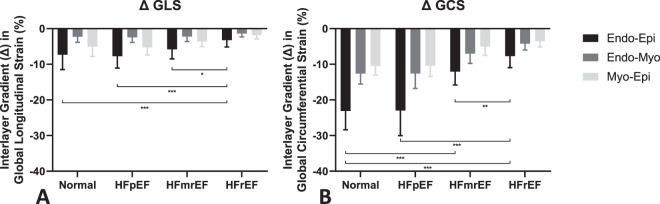
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
