

A novel method for internal fixation of basal fifth metatarsal fracture in athletes: a cadaveric study of the F.E.R.I. technique (Fifth metatarsal, Extra-portal, Rigid, Innovative)
- PMID: 31713049
- PMCID: PMC6848546
- DOI: 10.1186/s40634-019-0213-5
A novel method for internal fixation of basal fifth metatarsal fracture in athletes: a cadaveric study of the F.E.R.I. technique (Fifth metatarsal, Extra-portal, Rigid, Innovative)
Abstract
Purpose: One of the main problems of Kirschner wire fixation of fifth metatarsal base fractures (in combination with a tension band wiring technique) seems to be hardware intolerance and several studies in athletes also report failure after isolated fixation with a screw only. These reports prompted us to look at new materials and a novel technique through fixation with an intramedullary screw combined with a high-resistance suture via the presented F.E.R.I. (Fifth metatarsal, Extra-portal, Rigid, Innovative) technique.
Methods: This cadaveric study describes F.E.R.I.
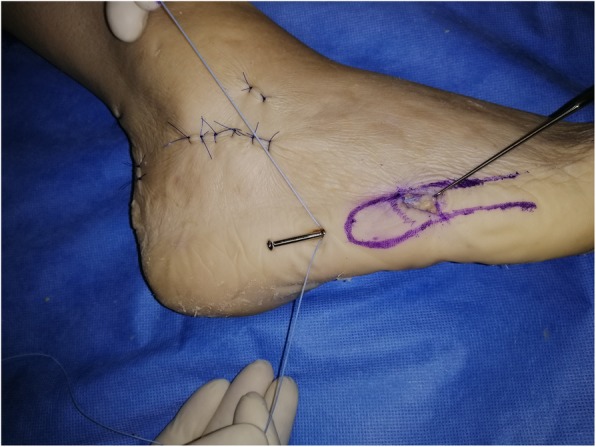
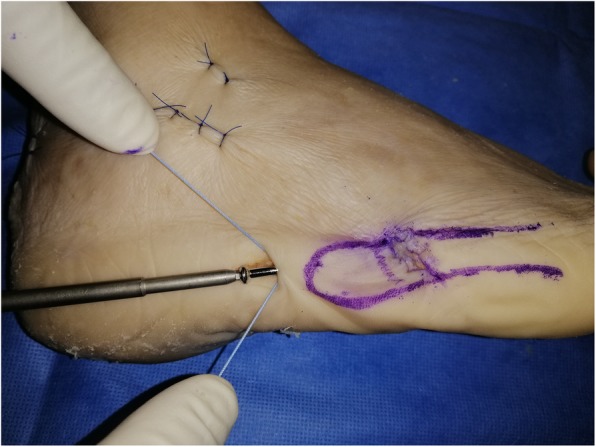
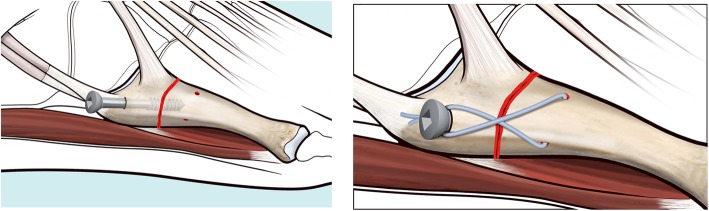
Technique: On a cadaver, through two mini portals, a full reduction and solid internal fixation with an intramedullary screw and suture cerclage with Fiberwire of a fifth metatarsal base fracture is achieved. In this article, the cadaveric study and proposed surgical technique are explained and illustrated step by step.
Results: The presented internal fixation F.E.R.I. technique is indicated in acute proximal fractures, stress fractures or non-union of metatarsal 5 (Zone 2-3 by Lawrence and Botte) and it resulted feasible and stable during manual stress test. The authors intend to study this technique in the clinical setting in the near future.
Conclusions: Fifth metatarsal base fractures gain specific interest when occurring in athletes. In this group of patients, internal fixation is often required to obtain a satisfactory outcome and time to return to play. The aim of the presented cadaveric study is to illustrate an innovative concept of internal fixation, named F.E.R.I.
Keywords: Athlete; Fifth metatarsal; Fracture; Internal fixation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Clapper M, O’Brien T, Lyons P. Fractures of the fifth metatarsal: analysis of a fracture registry. Clin Orthop Relat Res. 1995;315:238–241. - PubMed
LinkOut - more resources
Full Text Sources
