

Clinical Utility of Human Papillomavirus Genotyping in Cervical Cancer Screening: A Systematic Review
- PMID: 31714325
- PMCID: PMC6924950
- DOI: 10.1097/LGT.0000000000000494
Clinical Utility of Human Papillomavirus Genotyping in Cervical Cancer Screening: A Systematic Review
Abstract
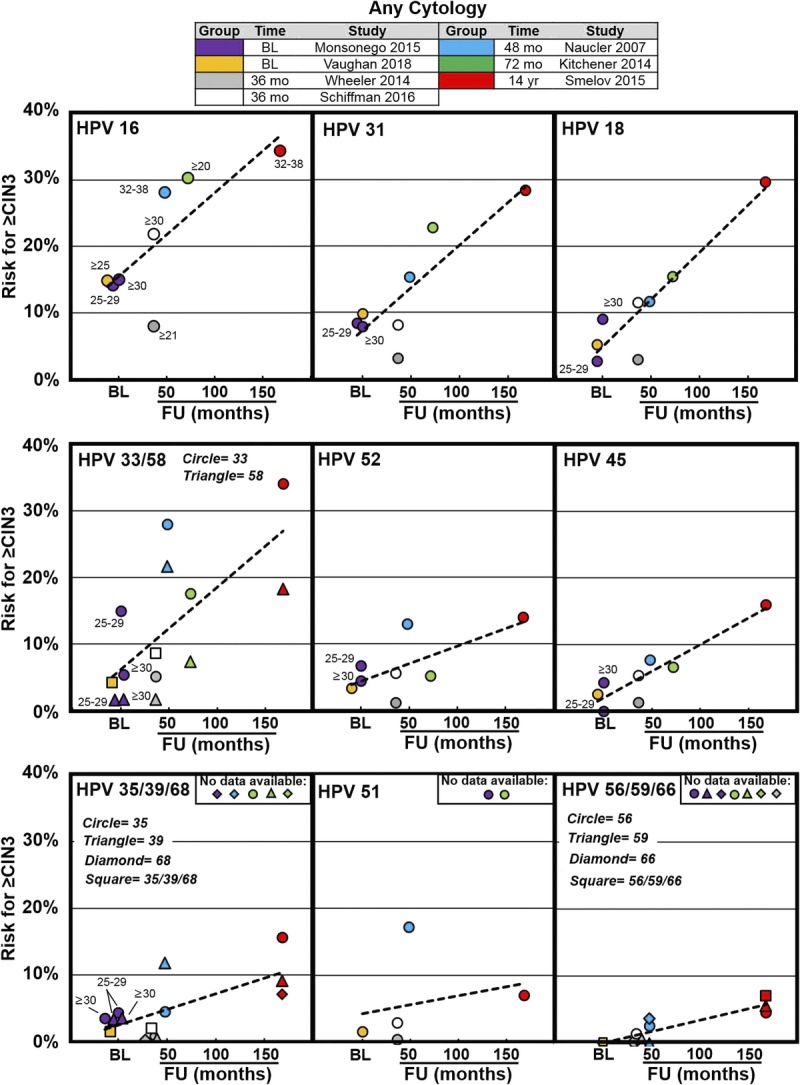
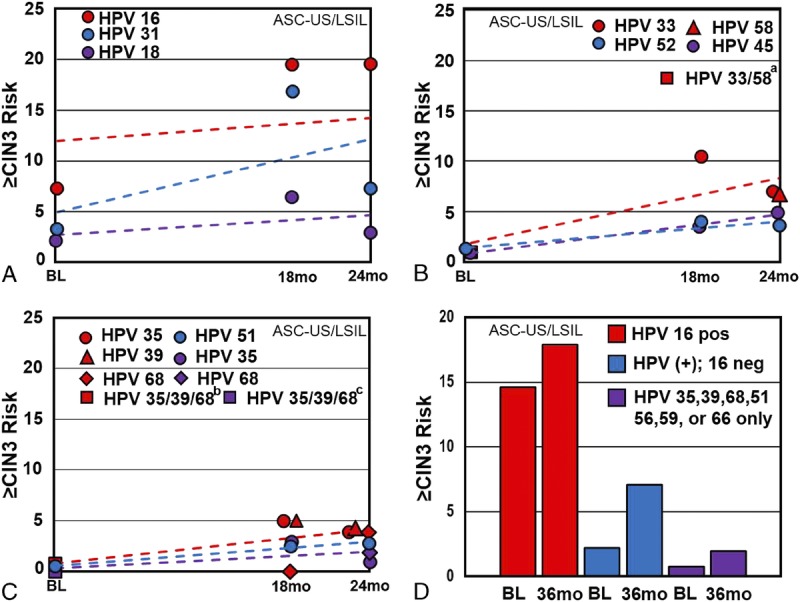
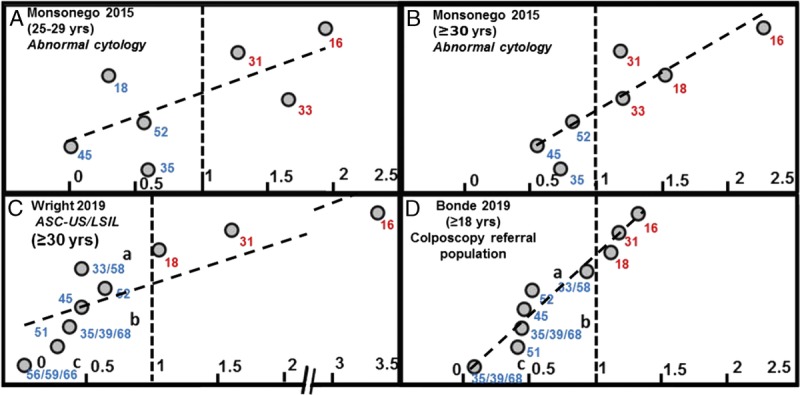
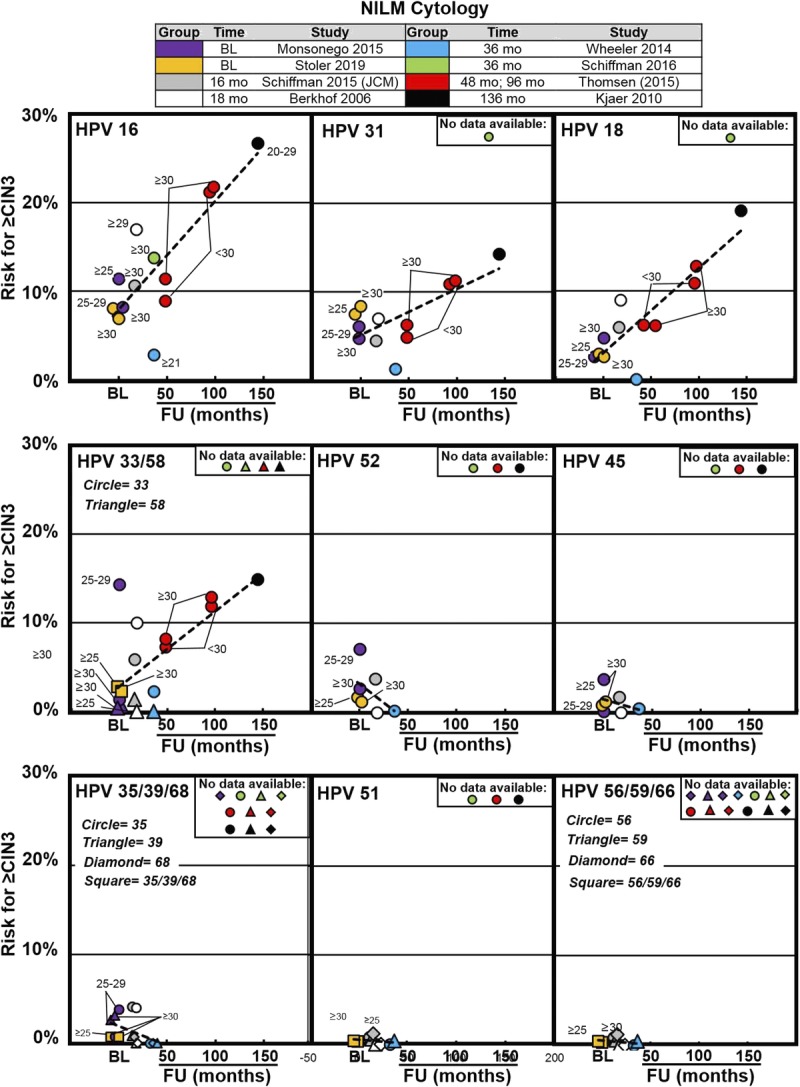
Objective: Thirteen human papillomavirus (HPV) genotypes are associated with the highest risk of cervical disease/cancer; however, the risk of disease progression and cancer is genotype dependent. The objective of this systematic review was to examine evidence for high-grade cervical intraepithelial neoplasia (≥CIN 3) risk discrimination using HPV genotyping.
Materials and methods: A systematic review of English and non-English articles through MEDLINE, Cochrane, clinicaltrials.gov, and abstracts presented at relevant professional society conferences were searched from 2000 to 2019. Search terms included: cervical cancer screening, HPV genotyping, CIN, HPV persistence, humans, and colposcopy; prospective, controlled trials, observational studies, and retrospective studies of residual specimens; evidence included HPV genotyping (beyond genotypes 16/18/45) results. Data were obtained independently by authors using predefined fields. Risk of bias was evaluated with a modified Newcastle-Ottawa Scale. The Grading of Recommendations, Assessment, Development and Evaluation methodology facilitated overall quality of evidence evaluation for risk estimation. The study protocol was registered with the PROSPERO International Prospective Register of Systematic Reviews (CRD42018091093). The primary outcome was CIN 3 or worse risk both at baseline and at different follow-up periods.
Results: Of 236 identified sources, 60 full texts were retrieved and 16 articles/sources were included. Risk of bias was deemed low; the overall quality of evidence for CIN 3 or worse risk with negative for intraepithelial lesions or malignancies or low-grade squamous intraepithelial cytology was assessed as moderate; that with atypical squamous cells-undetermined significance and "all cytology" was assessed as high. Clinical and methodological heterogeneity precluded meta-analysis. Human papillomavirus genotyping discriminated risk of CIN 3 or worse to a clinically significant degree, regardless of cytology result.
Conclusions: The evidence supports a clinical utility for HPV genotyping in risk discrimination during cervical cancer screening.
Figures
References
-
- de Villiers EM, Fauquet C, Broker TR, et al. Classification of papillomaviruses. Virology 2004;324:17–27. - PubMed
-
- de Sanjose S, Quint WG, Alemany L, et al. Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study. Lancet Oncol 2010;11:1048–56. - PubMed
-
- zur Hausen H. Similarities of papillomavirus infections with tumor promoters. Princess Takamatsu Symp 1983;14:147–52. - PubMed
-
- International Agency for Research on Cancer Human papillomaviruses. IARC Monogr Eval Carcinog Risks Hum 2012;100B:255–314.
