

Non-intubated anesthesia in patients undergoing video-assisted thoracoscopic surgery: A systematic review and meta-analysis
- PMID: 31714904
- PMCID: PMC6850529
- DOI: 10.1371/journal.pone.0224737
Non-intubated anesthesia in patients undergoing video-assisted thoracoscopic surgery: A systematic review and meta-analysis
Abstract
Introduction: Non-intubated anesthesia (NIA) has been proposed for video-assisted thoracoscopic surgery (VATS), although how the benefit-to-risk of NIA compares to that of intubated general anesthesia (IGA) for certain types of patients remains unclear. Therefore, the aim of the present meta-analysis was to understand whether NIA or IGA may be more beneficial for patients undergoing VATS.
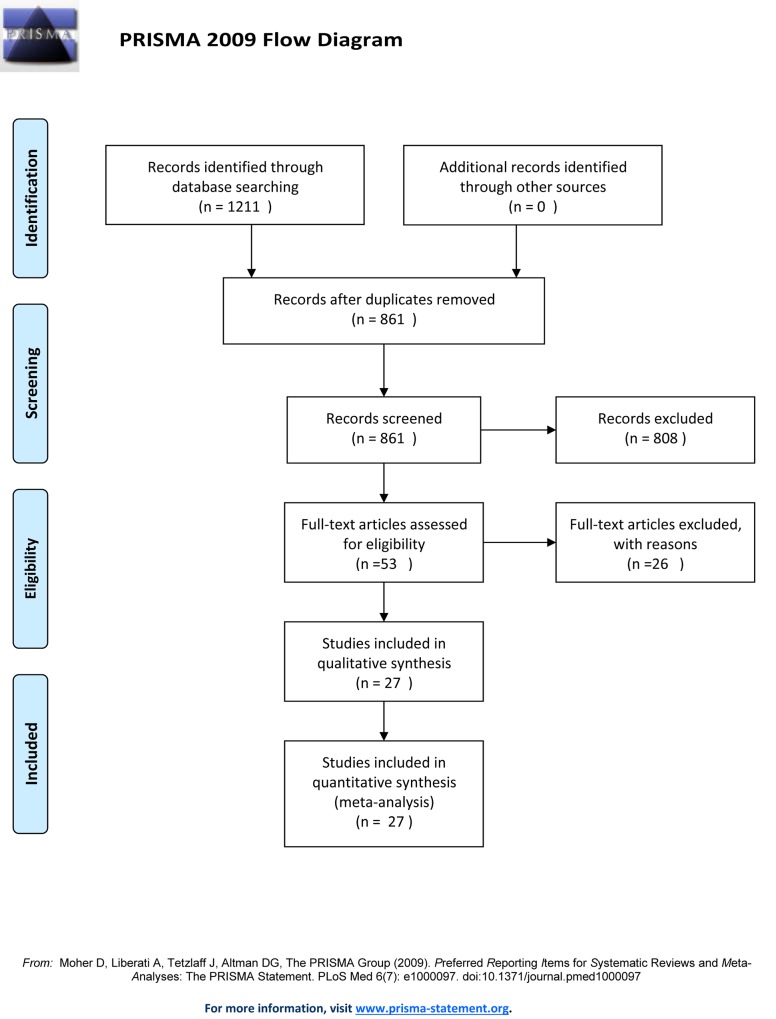
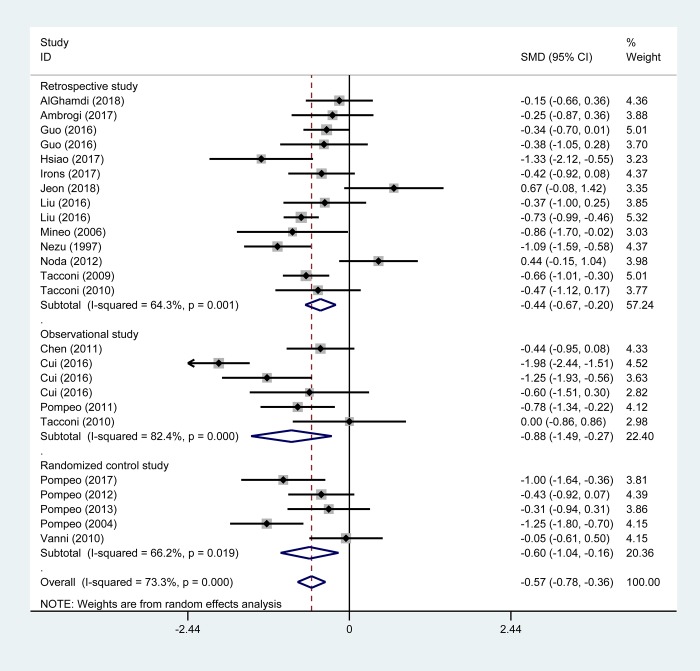
Methods: A systematic search of Cochrane Library, Pubmed and Embase databases from 1968 to April 2019 was performed using predefined criteria. Studies comparing the effects of NIA or IGA for adult VATS patients were considered. The primary outcome measure was hospital stay. Pooled data were meta-analyzed using a random-effects model to determine the standard mean difference (SMD) with 95% confidence intervals (CI).
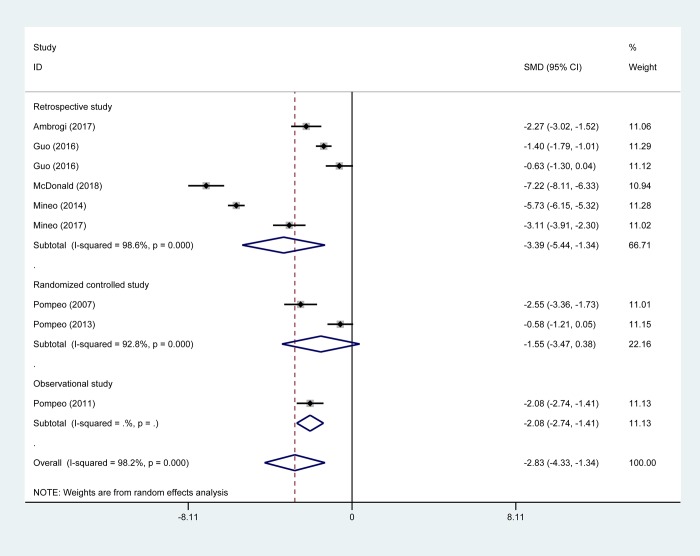
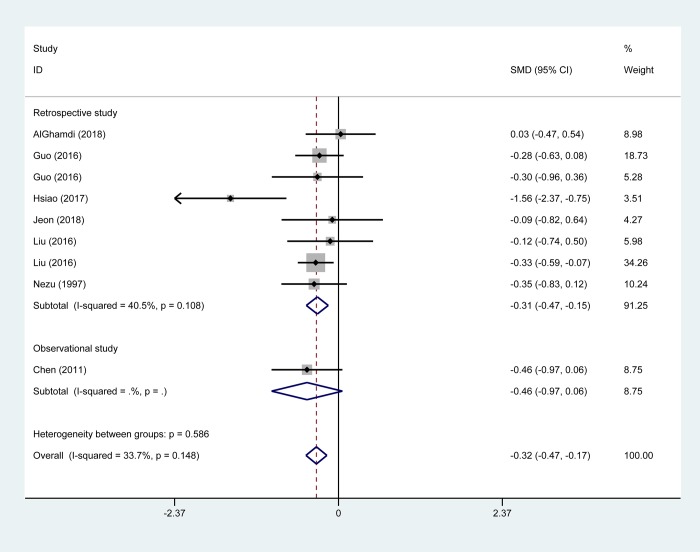
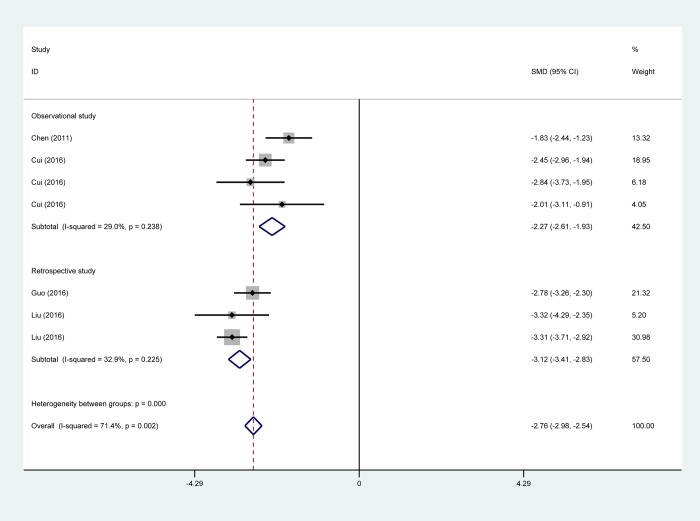
Results and discussion: Twenty-eight studies with 2929 patients were included. The median age of participants was 56.8 years (range 21.9-76.4) and 1802 (61.5%) were male. Compared to IGA, NIA was associated with shorter hospital stay (SMD -0.57 days, 95%CI -0.78 to -0.36), lower estimated cost for hospitalization (SMD -2.83 US, 95% CI -4.33 to -1.34), shorter chest tube duration (SMD -0.32 days, 95% CI -0.47 to -0.17), and shorter postoperative fasting time (SMD, -2.76 days; 95% CI -2.98 to -2.54). NIA patients showed higher levels of total lymphocytes and natural killer cells and higher T helper/T suppressor cell ratio, but lower levels of interleukin (IL)-6, IL-8 and C-reactive protein (CRP). Moreover, NIA patients showed lower levels of fibrinogen, cortisol, procalcitonin and epinephrine.
Conclusions: NIA enhances the recovery from VATS through attenuation of stress and inflammatory responses and stimulation of cellular immune function.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Non-intubated spontaneous ventilation in video-assisted thoracoscopic surgery: a meta-analysis.Eur J Cardiothorac Surg. 2020 Mar 1;57(3):428-437. doi: 10.1093/ejcts/ezz279. Eur J Cardiothorac Surg. 2020. PMID: 31725158
-
Non-intubated video-assisted thoracoscopic surgery under loco-regional anaesthesia for thoracic surgery: a meta-analysis.Interact Cardiovasc Thorac Surg. 2016 Jul;23(1):31-40. doi: 10.1093/icvts/ivw055. Epub 2016 Mar 16. Interact Cardiovasc Thorac Surg. 2016. PMID: 26984963 Free PMC article. Review.
-
Efficacy and Safety of Robot-assisted Thoracic Surgery (RATS) Compare with Video-assisted Thoracoscopic Surgery (VATS) for Lung Lobectomy in Patients with Non-small Cell Lung Cancer.Comb Chem High Throughput Screen. 2019;22(3):169-178. doi: 10.2174/1386207322666190411113040. Comb Chem High Throughput Screen. 2019. PMID: 30973106
-
[Video-assisted Thoracoscope versus Video-assisted Mini-thoracotomy for Non-small Cell Lung Cancer: A Meta-analysis].Zhongguo Fei Ai Za Zhi. 2017 May 20;20(5):303-311. doi: 10.3779/j.issn.1009-3419.2017.05.02. Zhongguo Fei Ai Za Zhi. 2017. PMID: 28532537 Free PMC article. Chinese.
-
Comparison of non-intubated and intubated video-assisted thoracoscopic surgery for perioperative complications-a systematic review and meta-analysis.BMC Anesthesiol. 2025 May 29;25(1):272. doi: 10.1186/s12871-025-03154-3. BMC Anesthesiol. 2025. PMID: 40442616 Free PMC article.
Cited by
-
Nonintubated versus Intubated Lung Volume Reduction Surgery in Patients with End-Stage Lung Emphysema and Hypercapnia.J Clin Med. 2023 May 29;12(11):3750. doi: 10.3390/jcm12113750. J Clin Med. 2023. PMID: 37297944 Free PMC article.
-
Pathophysiological Advantages of Spontaneous Ventilation.Front Surg. 2022 Mar 14;9:822560. doi: 10.3389/fsurg.2022.822560. eCollection 2022. Front Surg. 2022. PMID: 35360436 Free PMC article. Review.
-
The effect of different depths of anesthesia monitored using Narcotrend on cognitive function in elderly patients after VATS lobectomy.Am J Transl Res. 2021 Oct 15;13(10):11797-11805. eCollection 2021. Am J Transl Res. 2021. PMID: 34786108 Free PMC article.
-
A surgical Decision-making scoring model for spontaneous ventilation- and mechanical ventilation-video-assisted thoracoscopic surgery in non-small-cell lung cancer patients.BMC Surg. 2023 Sep 25;23(1):290. doi: 10.1186/s12893-023-02150-z. BMC Surg. 2023. PMID: 37743499 Free PMC article.
-
Case report: Simultaneous resections of pulmonary segment and an esophageal leiomyoma during spontaneous ventilation video-assisted thoracoscopic surgery.Front Oncol. 2024 May 21;14:1364306. doi: 10.3389/fonc.2024.1364306. eCollection 2024. Front Oncol. 2024. PMID: 38835375 Free PMC article.
References
-
- Bendixen M, Jorgensen OD, Kronborg C, Andersen C, Licht PB (2016) Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol 17: 836–844. 10.1016/S1470-2045(16)00173-X - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
