

High Clinical Value of Liquid Biopsy to Detect Circulating Tumor Cells and Tumor Exosomes in Pancreatic Ductal Adenocarcinoma Patients Eligible for Up-Front Surgery
- PMID: 31717747
- PMCID: PMC6895804
- DOI: 10.3390/cancers11111656
High Clinical Value of Liquid Biopsy to Detect Circulating Tumor Cells and Tumor Exosomes in Pancreatic Ductal Adenocarcinoma Patients Eligible for Up-Front Surgery
Abstract
Purpose: Expediting the diagnosis of pancreatic ductal adenocarcinoma (PDAC) would benefit care management, especially for the start of treatments requiring histological evidence. This study evaluated the combined diagnostic performance of circulating biomarkers obtained by peripheral and portal blood liquid biopsy in patients with resectable PDAC.
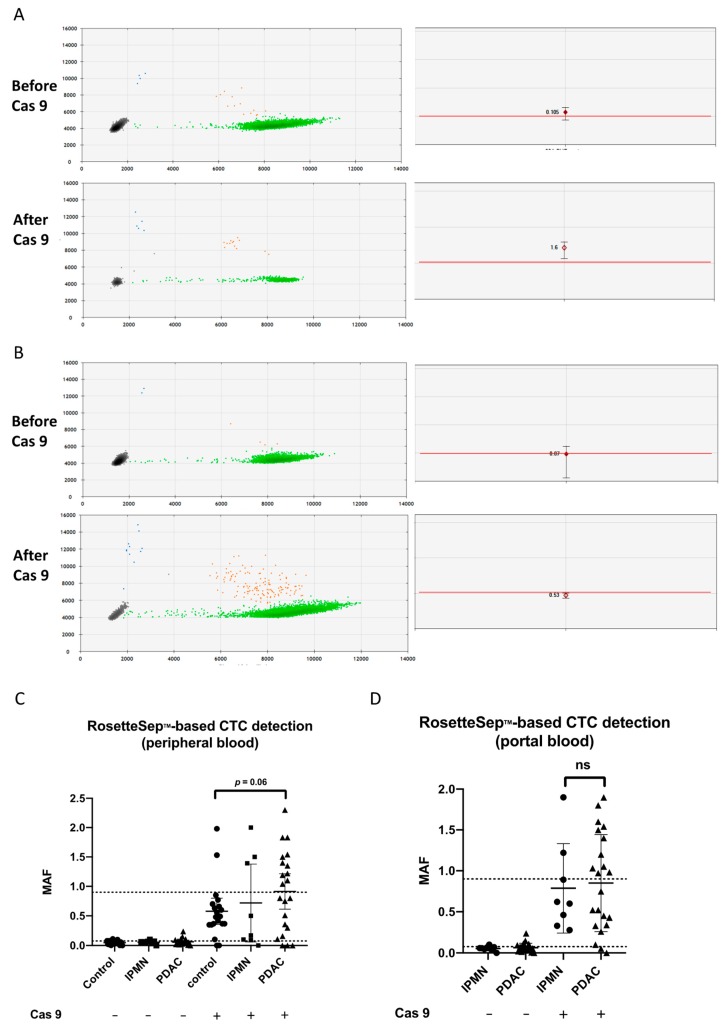
Experimental design: Liquid biopsies were performed in a prospective translational clinical trial (PANC-CTC #NCT03032913) including 22 patients with resectable PDAC and 28 noncancer controls from February to November 2017. Circulating tumor cells (CTCs) were detected using the CellSearch® method or after RosetteSep® enrichment combined with CRISPR/Cas9-improved KRAS mutant alleles quantification by droplet digital PCR. CD63 bead-coupled Glypican-1 (GPC1)-positive exosomes were quantified by flow cytometry.
Results: Liquid biopsies were positive in 7/22 (32%), 13/22 (59%), and 14/22 (64%) patients with CellSearch® or RosetteSep®-based CTC detection or GPC1-positive exosomes, respectively, in peripheral and/or portal blood. Liquid biopsy performance was improved in portal blood only with CellSearch®, reaching 45% of PDAC identification (5/11) versus 10% (2/22) in peripheral blood. Importantly, combining CTC and GPC1-positive-exosome detection displayed 100% of sensitivity and 80% of specificity, with a negative predictive value of 100%. High levels of GPC1+-exosomes and/or CTC presence were significantly correlated with progression-free survival and with overall survival when CTC clusters were found.
Conclusion: This study is the first to evaluate combined CTC and exosome detection to diagnose resectable pancreatic cancers. Liquid biopsy combining several biomarkers could provide a rapid, reliable, noninvasive decision-making tool in early, potentially curable pancreatic cancer. Moreover, the prognostic value could select patients eligible for neoadjuvant treatment before surgery. This exploratory study deserves further validation.
Keywords: circulating tumor cells; exosomes; liquid biopsy; pancreatic cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Tempero M.A., Malafa M.P., Al-Hawary M., Asbun H., Bain A., Behrman S.W., Benson A.B., Binder E., Cardin D.B., Cha C., et al. Pancreatic Adenocarcinoma, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN. 2017;15:1028–1061. doi: 10.6004/jnccn.2017.0131. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
