

Should All Patients With HR-Positive HER2-Negative Metastatic Breast Cancer Receive CDK 4/6 Inhibitor As First-Line Based Therapy? A Network Meta-Analysis of Data from the PALOMA 2, MONALEESA 2, MONALEESA 7, MONARCH 3, FALCON, SWOG and FACT Trials
- PMID: 31717791
- PMCID: PMC6896062
- DOI: 10.3390/cancers11111661
Should All Patients With HR-Positive HER2-Negative Metastatic Breast Cancer Receive CDK 4/6 Inhibitor As First-Line Based Therapy? A Network Meta-Analysis of Data from the PALOMA 2, MONALEESA 2, MONALEESA 7, MONARCH 3, FALCON, SWOG and FACT Trials
Abstract
Background: We aim to understand whether all patients with hormonal receptor (HR)-positive (+)/human epidermal growth factor receptor-2 (HER2)-negative (-) metastatic breast cancer (MBC) should receive cyclin D-dependent kinase (CDK) 4/6 inhibitor-based therapy as a first-line approach.
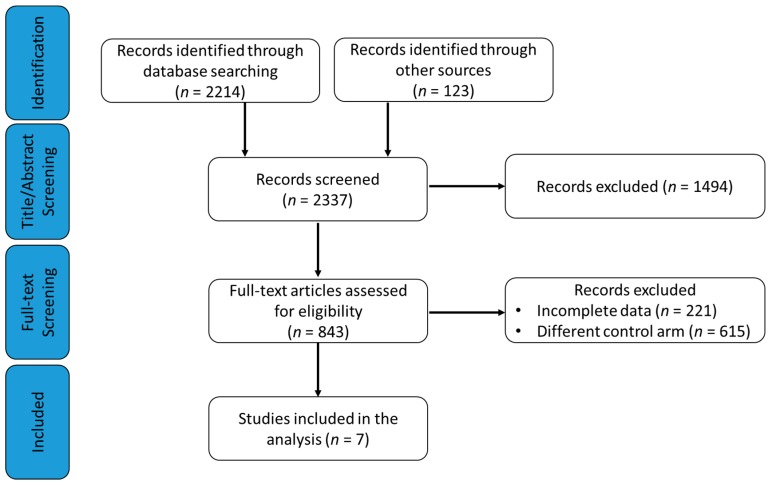
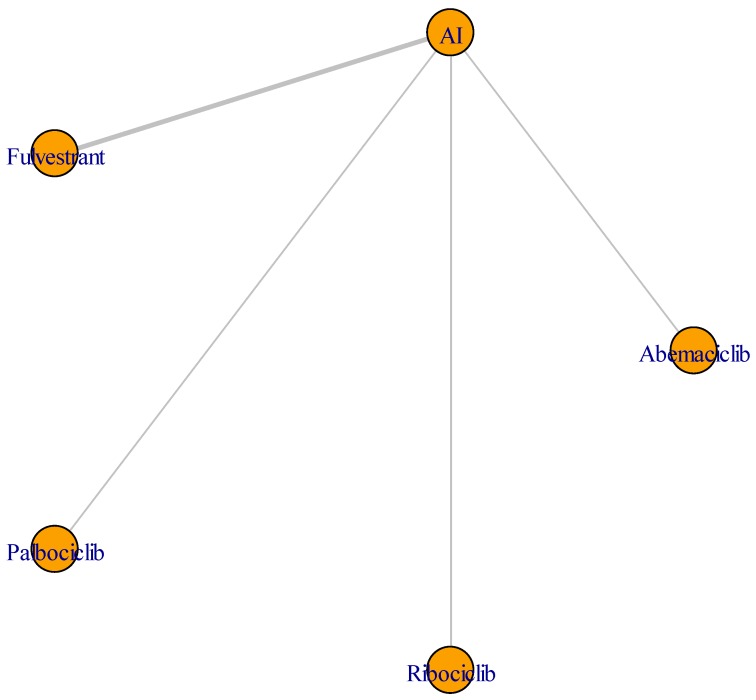
Methods: A network meta-analysis (NMA) using the Bayesian hierarchical arm-based model, which provides the estimates for various effect sizes, were computed.
Results: First-line treatment options in HR+/HER2- MBC, including CDK 4/6 inhibitors combined with aromatase inhibitors (AIs) or fulvestrant (F), showed a significantly longer progression-free survival (PFS) in comparison with AI monotherapy, with a total of 26% progression risk reduction. In the indirect comparison across the three classes of CDK 4/6 inhibitors and F endocrine-based therapies, the first strategy resulted in longer PFS, regardless of specific CDK 4/6 inhibitor (HR: 0.68; 95% CrI: 0.53-0.87 for palbociclib + AI, HR: 0.65; 95% CrI: 0.53-0.79 for ribociclib + AI, HR: 0.63; 95% CrI: 0.47-0.86 for abemaciclib + AI) and patient's characteristics. Longer PFS was also found in patients with bone-only and soft tissues limited disease treated with CDK 4/6 inhibitors.
Conclusions: CDK 4/6 inhibitors have similar efficacy when associated with an AI in the first-line treatment of HR+ MBC, and are superior to either F or AI monotherapy, regardless of any other patients or tumor characteristics.
Keywords: abemaciclib; aromatase inhibitors; fulvestrant; metastatic breast cancer; palbociclib; ribociclib.
Conflict of interest statement
E.B. received honoraria or speakers’ fee from MSD, Astra-Zeneca, Celgene, Pfizer, Helsinn, Eli-Lilly, BMS, Novartis, and Roche; E.B. is supported by the Associazione Italiana Ricerca Cancro (AIRC grants n. IG 20583). All other authors declare that they have no conflicts of interest.
Figures


References
-
- Sorlie T., Perou C.M., Tibshirani R., Aas T., Geisler S., Johnsen H., Hastie T., Eisen M.B., van de Rijn M., Jeffrey S.S., et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA. 2001;98:10869–10874. doi: 10.1073/pnas.191367098. - DOI - PMC - PubMed
-
- Rugo H.S., Rumble R.B., Macrae E., Barton D.L., Connolly H.K., Dickler M.N., Fallowfield L., Fowble B., Ingle J.N., Jahanzeb M., et al. Endocrine therapy for hormone receptor-positive metastatic breast cancer: American Society of Clinical Oncology Guideline. J. Clin. Oncol. 2016;34:3069–3103. doi: 10.1200/JCO.2016.67.1487. - DOI - PubMed
-
- Robertson J.F.R., Bondarenko I.M., Trishkina E., Dvorkin M., Panasci L., Manikhas A., Shparyk Y., Cardona-Huerta S., Cheung K.L., Philco-Salas M.J., et al. Fulvestrant 500 mg versus anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON): An international, randomised, double-blind, phase 3 trial. Lancet. 2016;388:2997–3005. doi: 10.1016/S0140-6736(16)32389-3. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
