

Tongue Rehabilitation Device for Dysphagic Patients
- PMID: 31717807
- PMCID: PMC6865205
- DOI: 10.3390/s19214657
Tongue Rehabilitation Device for Dysphagic Patients
Abstract
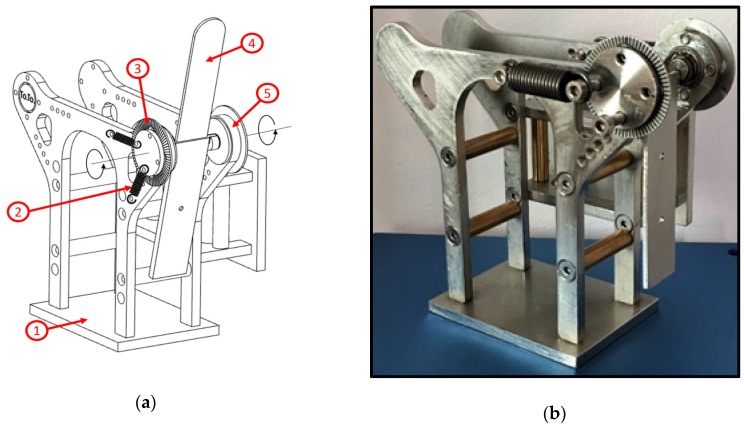
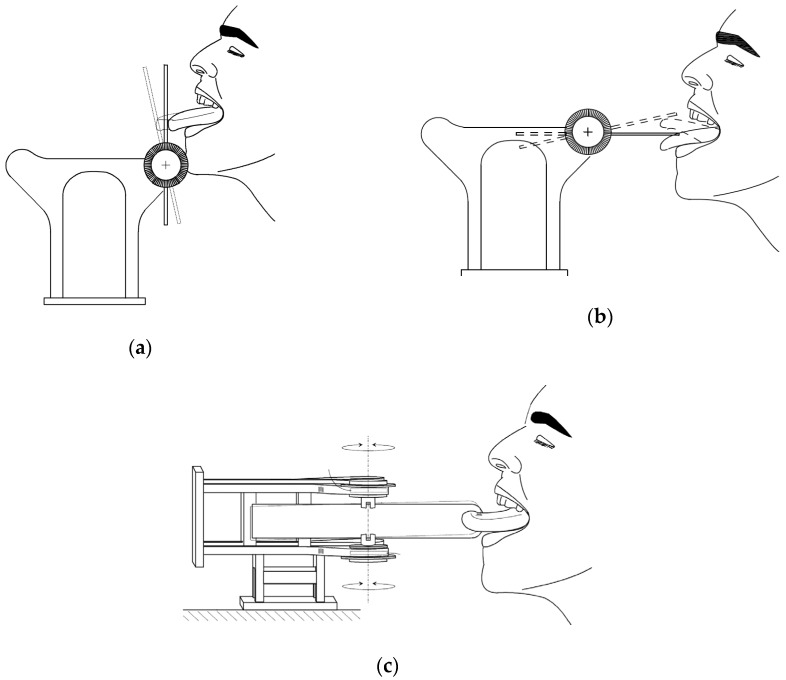
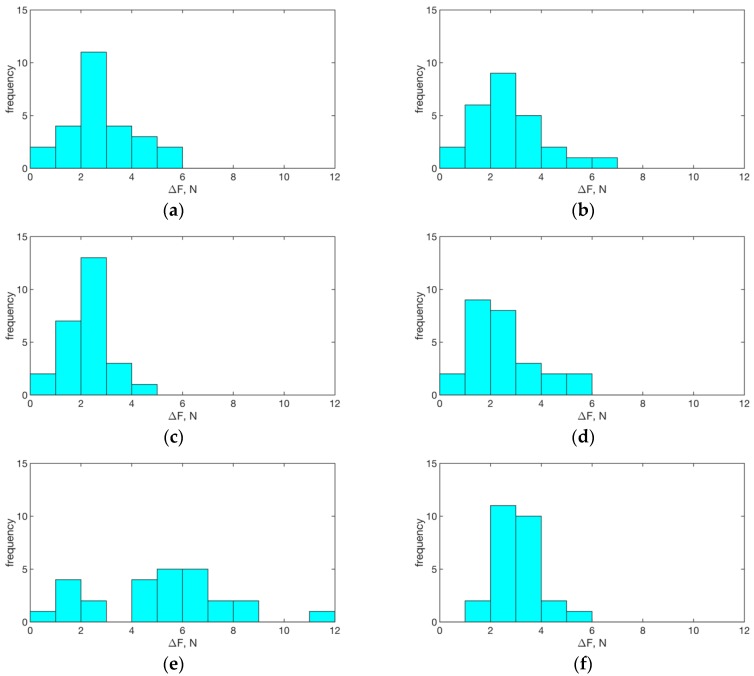
Dysphagia refers to difficulty in swallowing often associated with syndromic disorders. In dysphagic patients' rehabilitation, tongue motility is usually treated and monitored via simple exercises, in which the tongue is pushed against a depressor held by the speech therapist in different directions. In this study, we developed and tested a simple pressure/force sensor device, named "Tonic Tongue (ToTo)", intended to support training and monitoring tasks for the rehabilitation of tongue musculature. It consists of a metallic frame holding a ball bearing support equipped with a sterile disposable depressor, whose angular displacements are counterbalanced by extensional springs. The conversion from angular displacement to force is managed using a simple mechanical model of ToTo operation. Since the force exerted by the tongue in various directions can be estimated, quantitative assessment of the outcome of a given training program is possible. A first prototype of ToTo was tested on 26 healthy adults, who were trained for one month. After the treatment, we observed a statistically significant improvement with a force up to 2.2 N (median value) in all tested directions of pushing, except in the downward direction, in which the improvement was slightly higher than 5 N (median value). ToTo promises to be an innovative and reliable device that can be used for the rehabilitation of dysphagic patients. Moreover, since it is a self-standing device, it could be used as a point-of-care solution for in-home rehabilitation management of dysphasia.
Keywords: dysphagia; personalized medicine; rehabilitation; tongue.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Dotiwala A.K., Samra N.S. Anatomy, Head and Neck, Tongue. [(accessed on 10 September 2019)]; Available online: https://www.ncbi.nlm.nih.gov/books/NBK507782/
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
