

Diagnostic and prognostic value of interleukin-6, pentraxin 3, and procalcitonin levels among sepsis and septic shock patients: a prospective controlled study according to the Sepsis-3 definitions
- PMID: 31718563
- PMCID: PMC6852730
- DOI: 10.1186/s12879-019-4618-7
Diagnostic and prognostic value of interleukin-6, pentraxin 3, and procalcitonin levels among sepsis and septic shock patients: a prospective controlled study according to the Sepsis-3 definitions
Abstract
Background: This study investigated the clinical value of interleukin-6 (IL-6), pentraxin 3 (PTX3), and procalcitonin (PCT) in patients with sepsis and septic shock diagnosed according to the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).
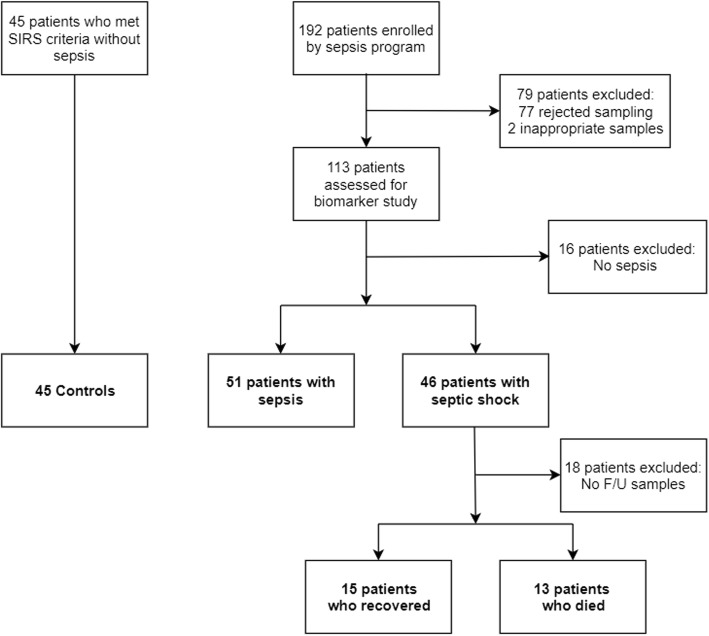
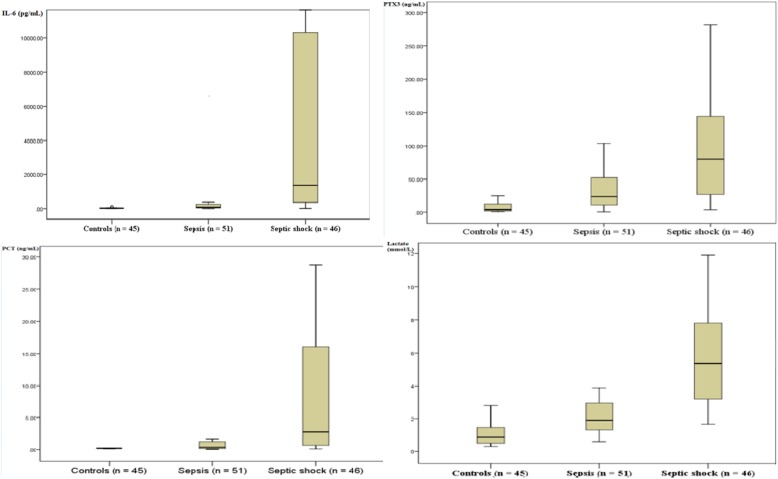
Methods: Serum levels of IL-6, PTX3, and PCT were measured in 142 enrolled subjects (51 with sepsis, 46 with septic shock, and 45 as controls). Follow-up IL-6 and PTX3 levels were measured in patients with initial septic shock within 24 h of hospital discharge. Optimal cut-off values were determined for sepsis and septic shock, and prognostic values were evaluated.
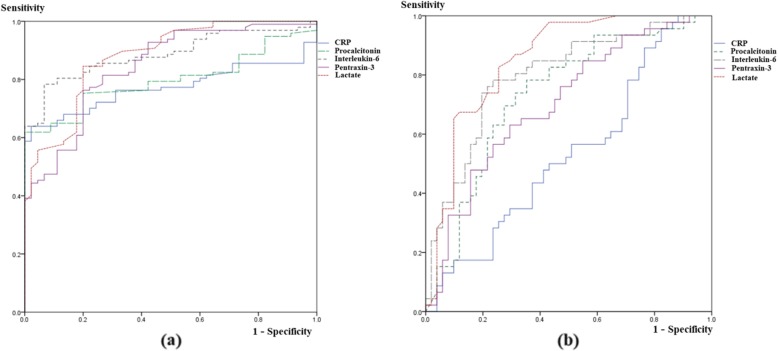
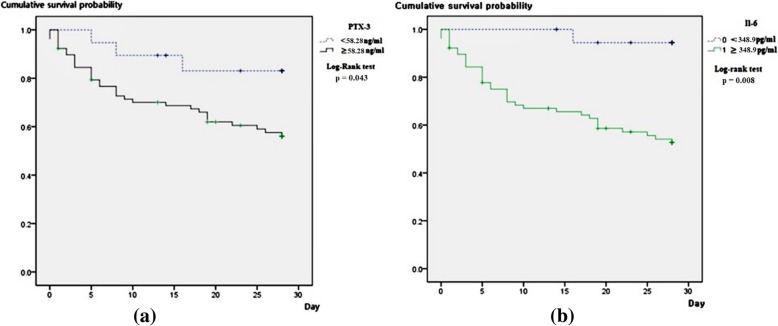
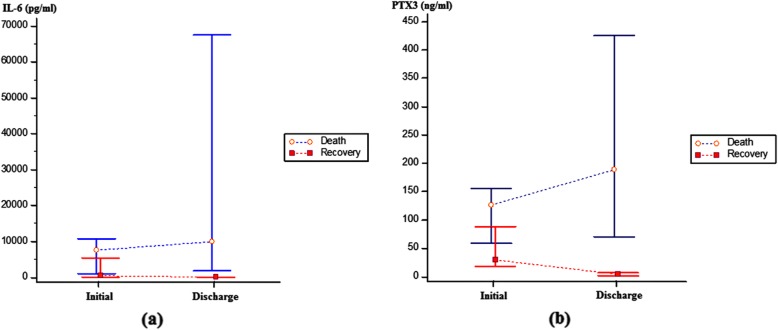
Results: Serum IL-6 levels could discriminate sepsis (area under the curve [AUC], 0.83-0.94, P < 0.001; cut-off value, 52.60 pg/mL, 80.4% sensitivity, 88.9% specificity) from controls and could distinguish septic shock (AUC, 0.71-0.89; cut-off value, 348.92 pg/mL, 76.1% sensitivity, 78.4% specificity) from sepsis. Twenty-eight-day mortality was significantly higher in the group with high IL-6 (≥ 348.92 pg/mL) than in the group with low IL-6 (< 348.92 pg/mL) (P = 0.008). IL-6 was an independent risk factor for 28-day mortality among overall patients (hazard ratio, 1.0004; 95% confidence interval, 1.0003-1.0005; p = 0.024). In septic shock patients, both the initial and follow-up PTX3 levels were consistently significantly higher in patients who died than in those who recovered (initial p = 0.004; follow-up P < 0.001).
Conclusions: The diagnostic and prognostic value of IL-6 was superior to those of PTX3 and PCT for sepsis and septic shock.
Keywords: Emergency department; Interleukin-6; Pentraxin 3; Procalcitonin; Sepsis; Septic shock.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Shankar-Hari M, Phillips GS, Levy ML, Seymour CW, Liu VX, Deutschman CS, et al. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for Sepsis and septic shock (Sepsis-3) JAMA. 2016;315(8):775–787. doi: 10.1001/jama.2016.0289. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
