

Long-term cognitive impairment after acute respiratory distress syndrome: a review of clinical impact and pathophysiological mechanisms
- PMID: 31718695
- PMCID: PMC6852966
- DOI: 10.1186/s13054-019-2626-z
Long-term cognitive impairment after acute respiratory distress syndrome: a review of clinical impact and pathophysiological mechanisms
Abstract
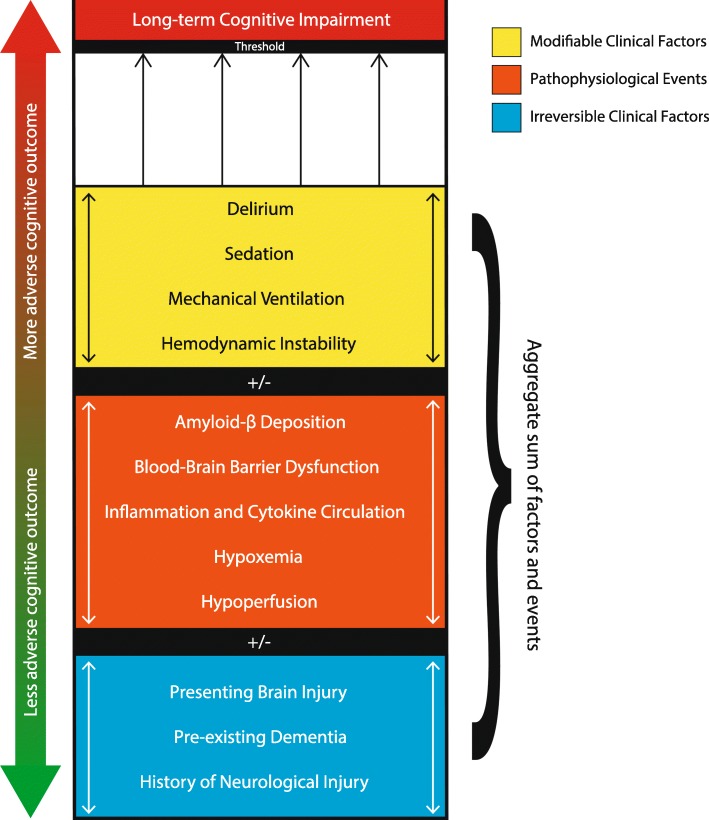
Acute respiratory distress syndrome (ARDS) survivors experience a high prevalence of cognitive impairment with concomitantly impaired functional status and quality of life, often persisting months after hospital discharge. In this review, we explore the pathophysiological mechanisms underlying cognitive impairment following ARDS, the interrelations between mechanisms and risk factors, and interventions that may mitigate the risk of cognitive impairment. Risk factors for cognitive decline following ARDS include pre-existing cognitive impairment, neurological injury, delirium, mechanical ventilation, prolonged exposure to sedating medications, sepsis, systemic inflammation, and environmental factors in the intensive care unit, which can co-occur synergistically in various combinations. Detection and characterization of pre-existing cognitive impairment imparts challenges in clinical management and longitudinal outcome study enrollment. Patients with brain injury who experience ARDS constitute a distinct population with a particular combination of risk factors and pathophysiological mechanisms: considerations raised by brain injury include neurogenic pulmonary edema, differences in sympathetic activation and cholinergic transmission, effects of positive end-expiratory pressure on cerebral microcirculation and intracranial pressure, and sensitivity to vasopressor use and volume status. The blood-brain barrier represents a physiological interface at which multiple mechanisms of cognitive impairment interact, as acute blood-brain barrier weakening from mechanical ventilation and systemic inflammation can compound existing chronic blood-brain barrier dysfunction from Alzheimer's-type pathophysiology, rendering the brain vulnerable to both amyloid-beta accumulation and cytokine-mediated hippocampal damage. Although some contributory elements, such as the presenting brain injury or pre-existing cognitive impairment, may be irreversible, interventions such as minimizing mechanical ventilation tidal volume, minimizing duration of exposure to sedating medications, maintaining hemodynamic stability, optimizing fluid balance, and implementing bundles to enhance patient care help dramatically to reduce duration of delirium and may help prevent acquisition of long-term cognitive impairment.
Keywords: ARDS; Blood-brain barrier; Cognitive impairment; ICU delirium; Inflammation; Mechanical ventilation; Outcomes; Pathophysiological mechanisms.
Conflict of interest statement
EWE: Pfizer and Orion honoraria for CME events. NIH and VA Funding. CS and SL declare that they have no competing interests.
Figures
Comment in
-
Mechanical ventilation and long-term neurocognitive impairment after acute respiratory distress syndrome.Crit Care. 2020 Jan 31;24(1):30. doi: 10.1186/s13054-020-2736-7. Crit Care. 2020. PMID: 32005278 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
