

Local Failure and Survival After Definitive Radiotherapy for Aggressive Prostate Cancer: An Individual Patient-level Meta-analysis of Six Randomized Trials
- PMID: 31718822
- PMCID: PMC7008470
- DOI: 10.1016/j.eururo.2019.10.008
Local Failure and Survival After Definitive Radiotherapy for Aggressive Prostate Cancer: An Individual Patient-level Meta-analysis of Six Randomized Trials
Abstract
Background: The importance of local failure (LF) after treatment of high-grade prostate cancer (PCa) with definitive radiotherapy (RT) remains unknown.
Objective: To evaluate the clinical implications of LF after definitive RT.
Design, setting, and participants: Individual patient data meta-analysis of 992 patients (593 Gleason grade group [GG] 4 and 399 GG 5) enrolled in six randomized clinical trials.
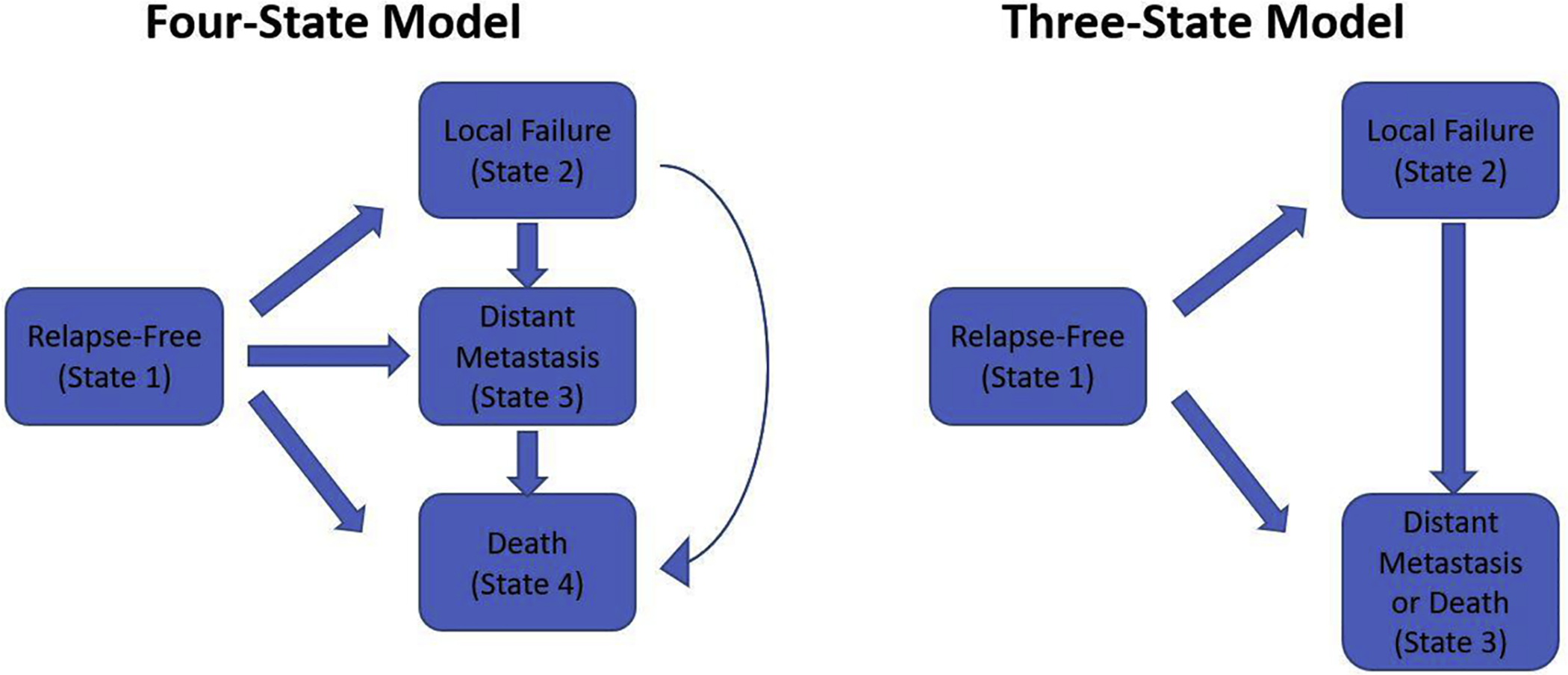
Outcome measurements and statistical analysis: Multivariable Cox proportional hazard models were developed to evaluate the relationship between overall survival (OS), PCa-specific survival (PCSS), and distant metastasis (DM)-free survival (DMFS) and LF as a time-dependent covariate. Markov proportional hazard models were developed to evaluate the impact of specific transitions between disease states on these endpoints.
Results and limitations: Median follow-up was 6.4 yr overall and 7.2 yr for surviving patients. LF was significantly associated with OS (hazard ratio [HR] 1.70 [95% confidence interval {CI} 1.37-2.10]), PCSS (3.10 [95% CI 2.33-4.12]), and DMFS (HR 1.92 [95% CI 1.54-2.39]), p < 0.001 for all). Patients who had not transitioned to the LF state had a significantly lower hazard of transitioning to a PCa-specific death state than those who transitioned to the LF state (HR 0.13 [95% CI 0.04-0.41], p < 0.001). Additionally, patients who transitioned to the LF state had a greater hazard of DM or death (HR 2.46 [95% CI 1.22-4.93], p = 0.01) than those who did not.
Conclusions: LF is an independent prognosticator of OS, PCSS, and DMFS in high-grade localized PCa and a subset of DM events that are anteceded by LF events. LF events warrant consideration for intervention, potentially suggesting a rationale for upfront treatment intensification. However, whether these findings apply to all men or just those without significant comorbidity remains to be determined.
Patient summary: Men who experience a local recurrence of high-grade prostate cancer after receiving upfront radiation therapy are at significantly increased risks of developing metastases and dying of prostate cancer.
Keywords: High grade; Local failure; Radiotherapy.
Copyright © 2019 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Local Failure in High-grade Prostate Cancer: An Elusive but Important Outcome and Target for Clinical Trials.Eur Urol. 2020 Feb;77(2):209-210. doi: 10.1016/j.eururo.2019.11.013. Epub 2019 Nov 29. Eur Urol. 2020. PMID: 31787428 No abstract available.
-
Local control matters.Transl Androl Urol. 2020 Jun;9(3):991-996. doi: 10.21037/tau-2020-06. Transl Androl Urol. 2020. PMID: 32676381 Free PMC article. No abstract available.
-
Implications of local failure on overall prognosis in aggressive prostate cancer.Transl Androl Urol. 2020 Jun;9(3):1001-1005. doi: 10.21037/tau-2020-04. Transl Androl Urol. 2020. PMID: 32676383 Free PMC article. No abstract available.
References
-
- Fossa SD, Wiklund F, Klepp O, et al. Ten- and 15-yr prostate cancer-specific mortality in patients with nonmetastatic locally advanced or aggressive intermediate prostate cancer, randomized to lifelong endocrine treatment alone or combined with radiotherapy: final results of the Scandinavian Prostate Cancer Group-7. Eur Urol 2016;70:684–91. - PubMed
-
- Grossman HB, Batata M, Hilaris B, Whitmore WF Jr. 125I implantation for carcinoma of prostate. Further follow-up of first 100 cases. Urology 1982;20:591–8. - PubMed
-
- Coen JJ, Zietman AL, Thakral H, Shipley WU. Radical radiation for localized prostate cancer: local persistence of disease results in a late wave of metastases. J Clin Oncol 2002;20:3199–205. - PubMed
-
- Freiha FS, Bagshaw MA. Carcinoma of the prostate: results of post-irradiation biopsy. Prostate 1984;5:19–25. - PubMed
