

Dissociable neural substrates of opioid and cocaine use identified via connectome-based modelling
- PMID: 31719641
- PMCID: PMC7214212
- DOI: 10.1038/s41380-019-0586-y
Dissociable neural substrates of opioid and cocaine use identified via connectome-based modelling
Abstract
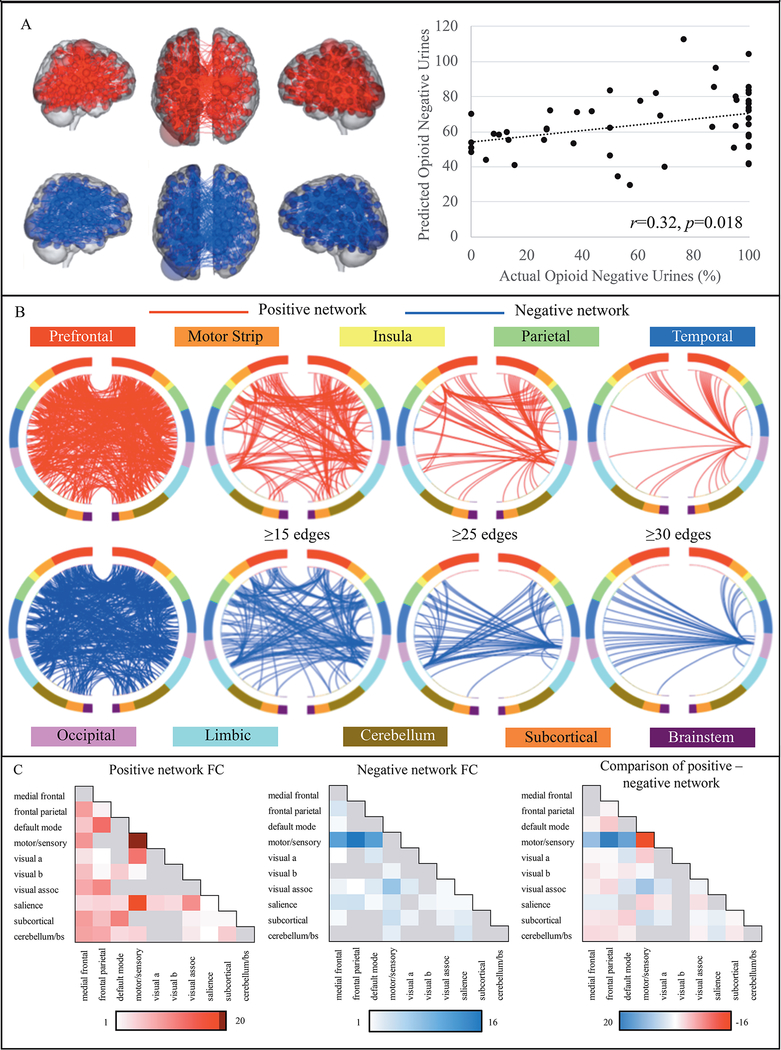
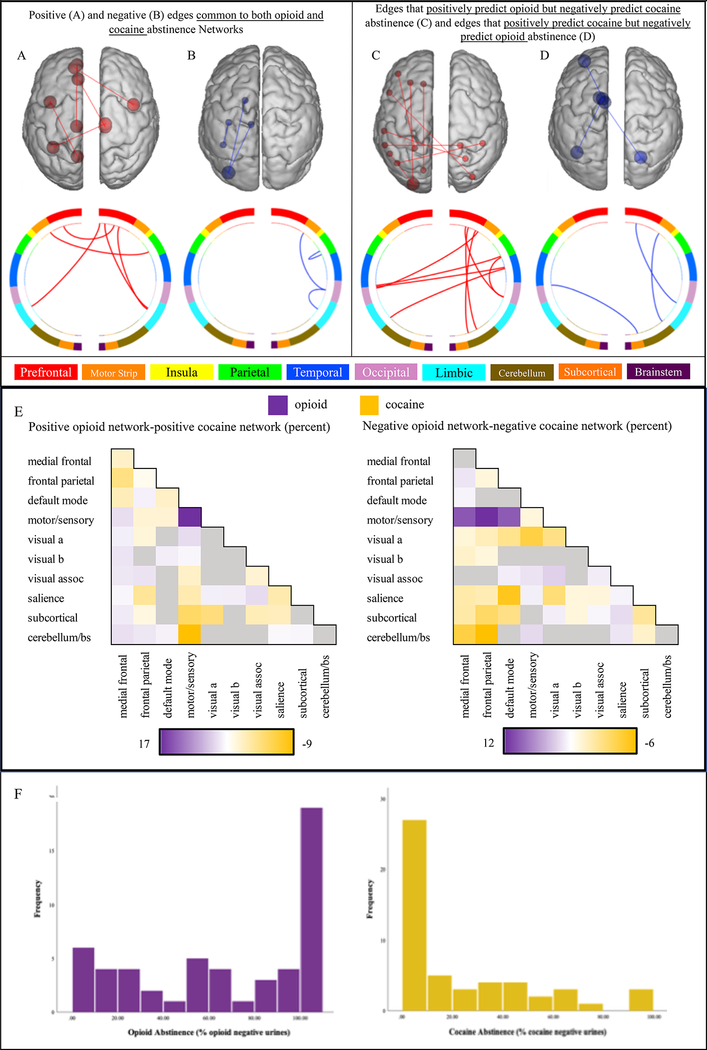
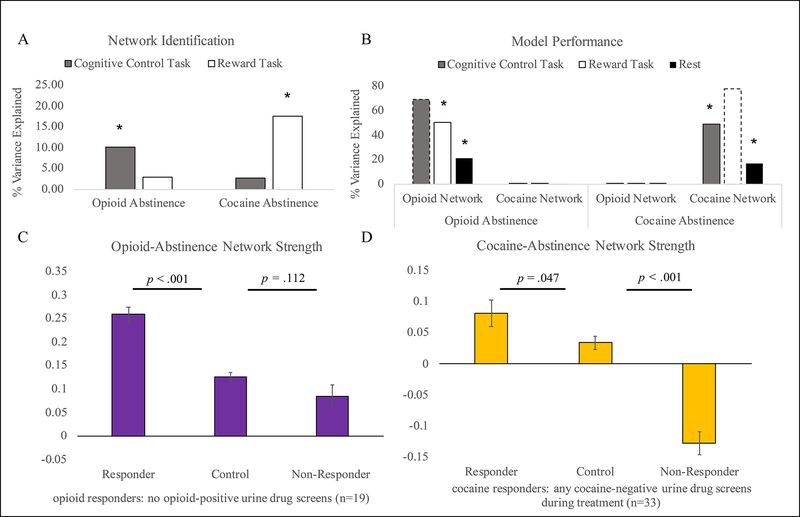
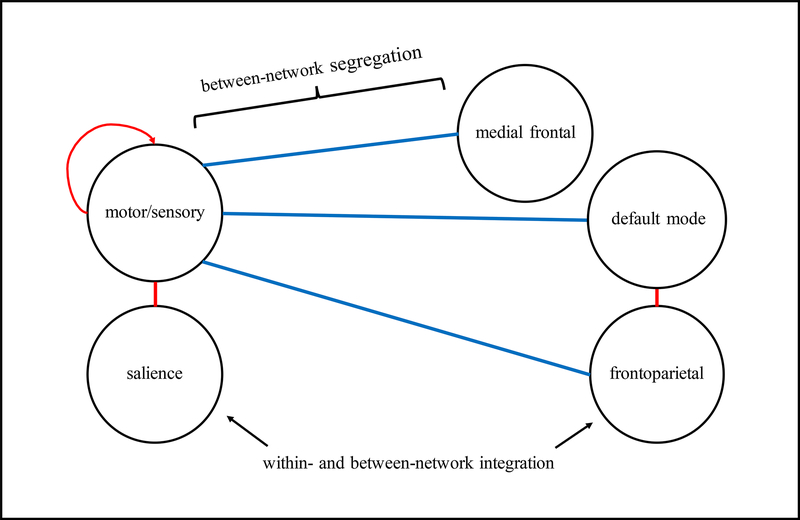
Opioid use disorder is a major public health crisis. While effective treatments are available, outcomes vary widely across individuals and relapse rates remain high. Understanding neural mechanisms of treatment response may facilitate the development of personalized and/or novel treatment approaches. Methadone-maintained, polysubstance-using individuals (n = 53) participated in fMRI scanning before and after substance-use treatment. Connectome-based predictive modeling (CPM)-a recently developed, whole-brain approach-was used to identify pretreatment connections associated with abstinence during the 3-month treatment. Follow-up analyses were conducted to determine the specificity of the identified opioid abstinence network across different brain states (cognitive vs. reward task vs. resting-state) and different substance use outcomes (opioid vs. cocaine abstinence). Posttreatment fMRI data were used to assess network changes over time and within-subject replication. To determine further clinical relevance, opioid abstinence network strength was compared with healthy subjects (n = 38). CPM identified an opioid abstinence network (p = 0.018), characterized by stronger within-network motor/sensory connectivity, and reduced connectivity between the motor/sensory network and medial frontal, default mode, and frontoparietal networks. This opioid abstinence network was anatomically distinct from a previously identified cocaine abstinence network. Relationships between abstinence and opioid and cocaine abstinence networks replicated across multiple brain states but did not generalize across substances. Network connectivity measured at posttreatment related to abstinence at 6-month follow-up (p < 0.009). Healthy comparison subjects displayed intermediate network strengths relative to treatment responders and nonresponders. These data indicate dissociable anatomical substrates of opioid vs. cocaine abstinence. Results may inform the development of novel opioid-specific treatment approaches to combat the opioid epidemic.
© 2019. The Author(s), under exclusive licence to Springer Nature Limited.
Figures
References
-
- Van den Brink W, Haasen C. Evidenced-based treatment of opioid-dependent patients. Can J Psychiatry 2006; 51(10): 635–646. - PubMed
-
- Connery HS. Medication-assisted treatment of opioid use disorder: review of the evidence and future directions. Harv Rev Psychiatry 2015; 23(2): 63–75. - PubMed
-
- Moningka H, Lichenstein S, Worhunsky PD, DeVito EE, Scheinost D, Yip SW. Can neuroimaging help combat the opioid epidemic? A systematic review of clinical and pharmacological challenge fMRI studies with recommendations for future research. Neuropsychopharmacology 2019; 44(2): 259–273. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
