

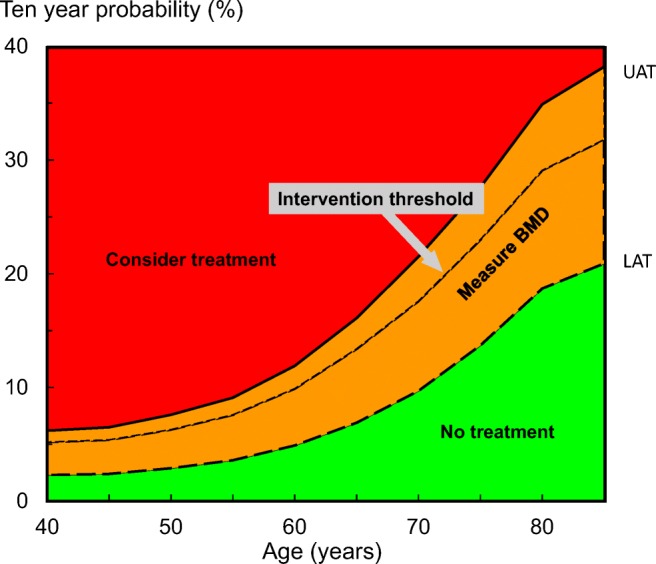
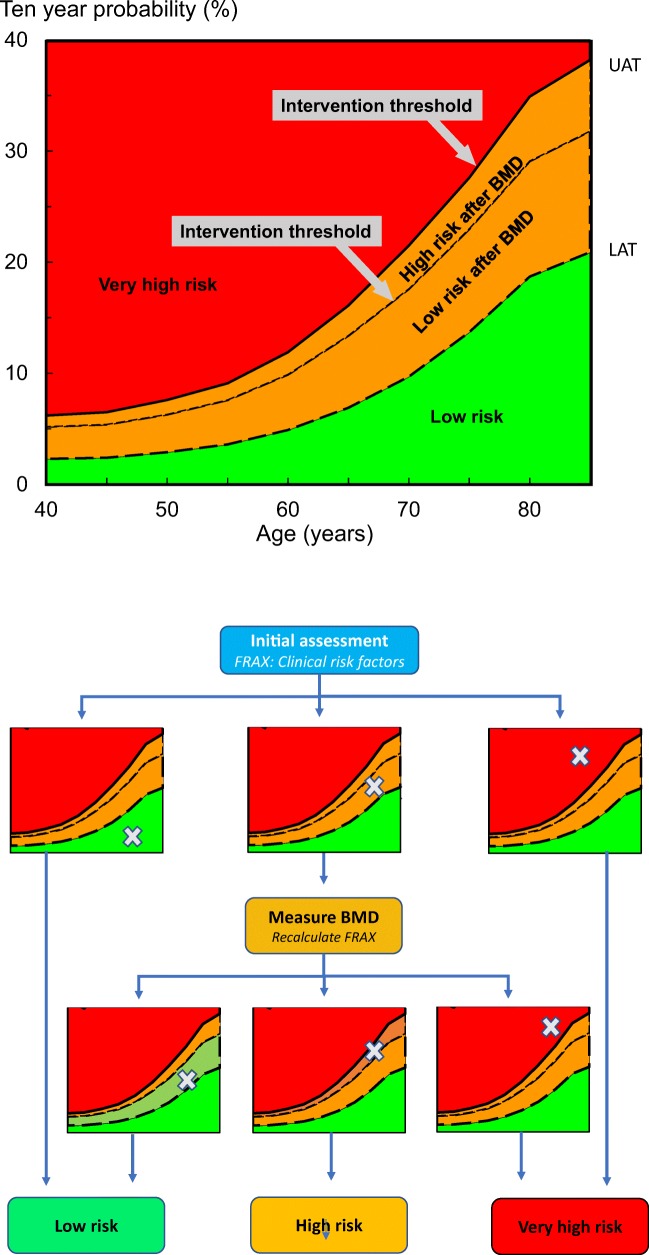
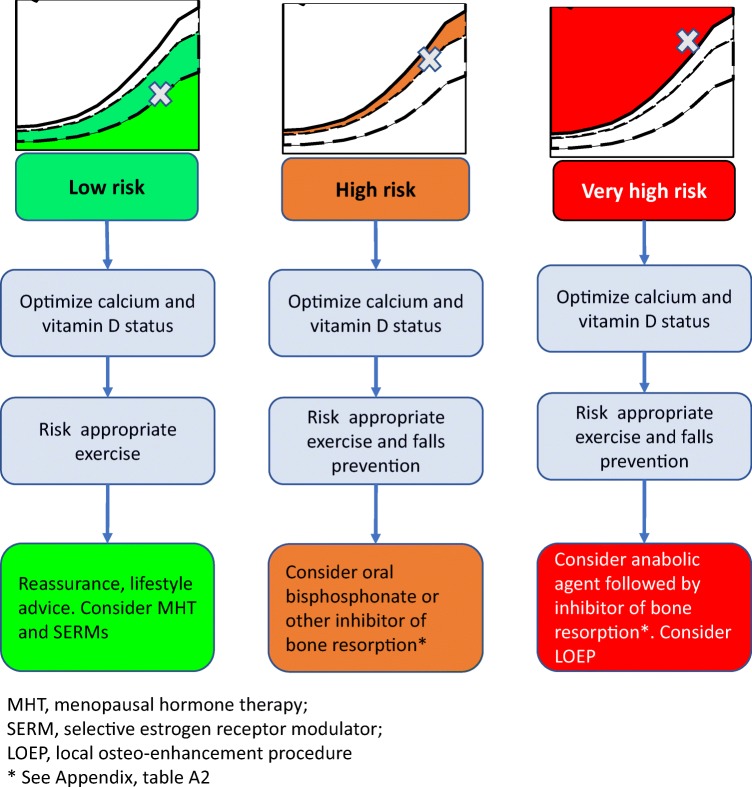
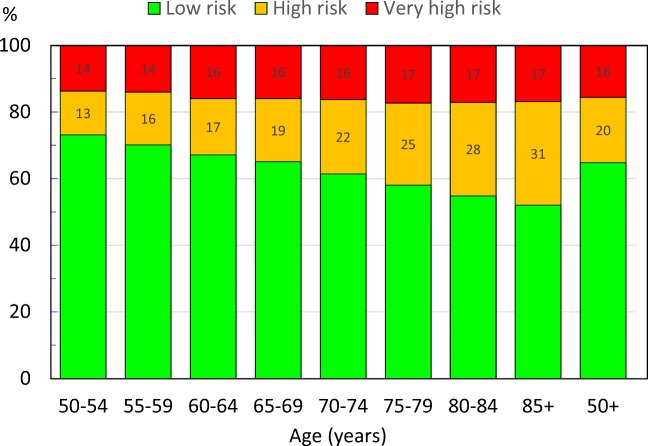
Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures
- PMID: 31720707
- PMCID: PMC7018677
- DOI: 10.1007/s00198-019-05176-3
Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures
Erratum in
-
Correction to: Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures.Osteoporos Int. 2020 Apr;31(4):797-798. doi: 10.1007/s00198-020-05297-0. Osteoporos Int. 2020. PMID: 32065251 Free PMC article.
Abstract
Guidance is provided in an international setting on the assessment and specific treatment of postmenopausal women at low, high and very high risk of fragility fractures.
Introduction: The International Osteoporosis Foundation and European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis published guidance for the diagnosis and management of osteoporosis in 2019. This manuscript seeks to apply this in an international setting, taking additional account of further categorisation of increased risk of fracture, which may inform choice of therapeutic approach.
Methods: Clinical perspective and updated literature search.
Results: The following areas are reviewed: categorisation of fracture risk and general pharmacological management of osteoporosis.
Conclusions: A platform is provided on which specific guidelines can be developed for national use to characterise fracture risk and direct interventions.
Keywords: Anabolic agents; FRAX; Fracture risk assessment; Inhibitors of bone resorption; Treatment of osteoporosis.
Conflict of interest statement
NM Al-Daghri G Adib, C Campusano, M Chandran, F Jiwa, H Johansson, JK Lee, E Liu, D Pinto, N Veronese, W Xia, L Zakraoui have no conflicts of interest to declare.
O Bruyère received research grants from Biophytis, IBSA, MEDA, Servier and SMB and consulting or lecture fees from Amgen, Biophytis, IBSA, MEDA, Servier, SMB, TRB Chemedica and UCB.
C Cooper reports personal fees from Alliance for Better Bone Health, Amgen, Eli Lilly, GSK, Medtronic, Merck, Novartis, Pfizer, Roche, Servier, Takeda and UCB.
B. Dawson-Hughes has received grant support from Pfizer and DSM and consulting fees from TTY Biopharma Co, Ltd, Intrinsic Therapeutics and Agnovos.
NC Harvey has received consultancy/lecture fees/honoraria/grant funding from Alliance for Better Bone Health, Amgen, MSD, Eli Lilly, Radius Health, Servier, Shire, UCB, Consilient Healthcare and Internis Pharma.
MK Javaid has received honoraria, unrestricted research grants, travel and/or subsistence expenses from Amgen, Lilly UK, Internis, Consilient Health, Zebra Medical Vision, Kyowa Kirin Hakin and UCB.
JA Kanis reports grants from Amgen, Eli Lilly and Radius Health and consulting fees from Theramex. JAK is the architect of FRAX® but has no financial interest.
M Lorentzon has received lecture fees from Amgen, Lilly, Meda, Renapharma and UCB Pharma and consulting fees from Amgen, Radius Health, UCB Pharma, Renapharma and Consilient Health, all outside the presented work.
EV McCloskey has received consultancy/lecture fees/grant funding/honoraria from ActiveSignal, AgNovos, Amgen, AstraZeneca, Consilient Healthcare, Fresenius Kabi, Gilead, GSK, Hologic, Internis, Lilly, Medtronic, Merck, Novartis, Pfizer, Radius Health, Redx Oncology, Roche, SanofiAventis, Servier, Synexus, Tethys, UCB, Viiv, Warner Chilcott, I3 Innovus and Unilever.
OD Messina has received honoraria from Amgen, Lilly, Novartis and Pfizer
O Minski received honorary fees for lectures, from Abbvie, Roche, Pfizer, Pierre Fabre, Janssen, Novartis and MSD.
D Prieto-Alhambra’s research group has received research grants from Amgen, Servier and UCB; speaker fees from Amgen and UCB; educational grants from Johnson & Johnson and consultancy fees from Amgen and UCB.
J-Y Reginster has received advisory board or consulting fees from IBSA-Genévrier, Pierre Fabre, Radius Health, TEVA and Mylan; lecture fees from Agnovos, IBSA-Genévrier, Mylan, CNIEL, Dairy Research Council (DRC) and Theramex and institutional grant support from IBSA-Genévrier, Mylan, CNIEL and Radius Health.
R Rizzoli has received consulting fees or advisory board fees from Radius Health, Labatec, Danone, Nestlé, CNIEL and Sandoz.
K Saag reports grant support from Amgen and Radius and consulting fees from Amgen, Radius and Roche.
Figures
Comment in
-
Comments on Kanis et al.: Algorithm for the management of patients at low, high, and very high risk of osteoporotic fractures.Osteoporos Int. 2020 May;31(5):1015. doi: 10.1007/s00198-020-05302-6. Epub 2020 Jan 17. Osteoporos Int. 2020. PMID: 31953592 No abstract available.
References
-
- Kanis JA, Cooper C, Rizzoli R, Reginster J-Y, Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019;30:3–44. - PMC - PubMed
-
- Kanis JA, Cooper C, Rizzoli R, Reginster J-Y. Executive summary of European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Aging Clin Exp Res. 2019;31:15–17. - PubMed
-
- Johnell O, Oden A, Caulin F, Kanis JA. Acute and long-term increase in fracture risk after hospitalization for vertebral fracture. Osteoporos Int. 2001;12:207–214. - PubMed
-
- Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I, Pettersen C, De Laet C, Jonsson B. Fracture risk following an osteoporotic fracture. Osteoporos Int. 2004;15:175–179. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
