

Association of Punitive and Reporting State Policies Related to Substance Use in Pregnancy With Rates of Neonatal Abstinence Syndrome
- PMID: 31722022
- PMCID: PMC6902764
- DOI: 10.1001/jamanetworkopen.2019.14078
Association of Punitive and Reporting State Policies Related to Substance Use in Pregnancy With Rates of Neonatal Abstinence Syndrome
Abstract
Importance: Despite the rapidly changing policy environment regarding substance use during pregnancy, information is lacking on the association of state policies with neonatal abstinence syndrome (NAS).
Objective: To determine if punitive or reporting state policies related to substance use during pregnancy are associated with NAS rates.
Design, setting, and participants: This repeated cross-sectional study used retrospective, difference-in-difference analysis of live births in the State Inpatient Databases from 8 US states in varying years between January 1, 2003, and December 31, 2014. States without punitive or reporting policies were compared with states with policies before and after policy enactment using logistic regression models adjusted for individual and county-level factors and state and year fixed effects. Analyses were conducted from April 10, 2019, to July 30, 2019.
Exposures: Time since enactment of state policies related to substance use in pregnancy, county-level rurality and unemployment, and presence of specialized treatment programs for pregnant and postpartum women in a county.
Main outcome and measures: Rates of NAS.
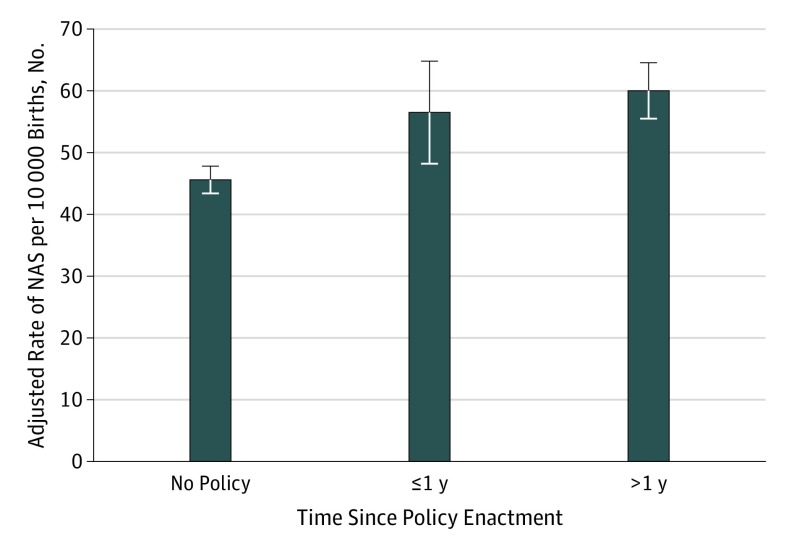
Results: Among 4 567 963 live births, 23 377 neonates (0.5%) received a diagnosis of NAS. Among neonates with NAS, 3394 (14.5%) lived in counties without any treatment programs specifically for pregnant and postpartum women, 20 323 (86.9%) lived in metropolitan counties, and 8135 (34.8%) lived in counties in the highest unemployment quartile. In adjusted analyses among neonates in states with punitive policies, odds of NAS were significantly greater during the first full calendar year after enactment (adjusted odds ratio, 1.25; 95% CI, 1.06-1.46; P = .007) and more than 1 full year after enactment (adjusted odds ratio, 1.33; 95% CI, 1.17-1.51; P < .001). After regression adjustment, the annual NAS rate was 46 (95% CI, 43-48) neonates with NAS per 10 000 live births in states without punitive policies; 57 (95% CI, 48-65) neonates with NAS per 10 000 live births in states with punitive policies during the first full year after enactment; and 60 (95% CI, 56-65) neonates with NAS per 10 000 live births in states with punitive policies in effect for more than 1 full year. There was no association between reporting policies and odds of NAS.
Conclusions and relevance: In this repeated cross-sectional analysis of 8 states, states with punitive policies were associated with greater odds of NAS immediately and in the longer term, but there was no association between NAS and states with reporting policies.
Conflict of interest statement
Figures
Comment in
-
It's Time to Support, Rather Than Punish, Pregnant Women With Substance Use Disorder.JAMA Netw Open. 2019 Nov 1;2(11):e1914135. doi: 10.1001/jamanetworkopen.2019.14135. JAMA Netw Open. 2019. PMID: 31722020 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
