

Right Ventricular Outflow Doppler Predicts Low Cardiac Index in Intermediate Risk Pulmonary Embolism
- PMID: 31722539
- PMCID: PMC7019409
- DOI: 10.1177/1076029619886062
Right Ventricular Outflow Doppler Predicts Low Cardiac Index in Intermediate Risk Pulmonary Embolism
Abstract
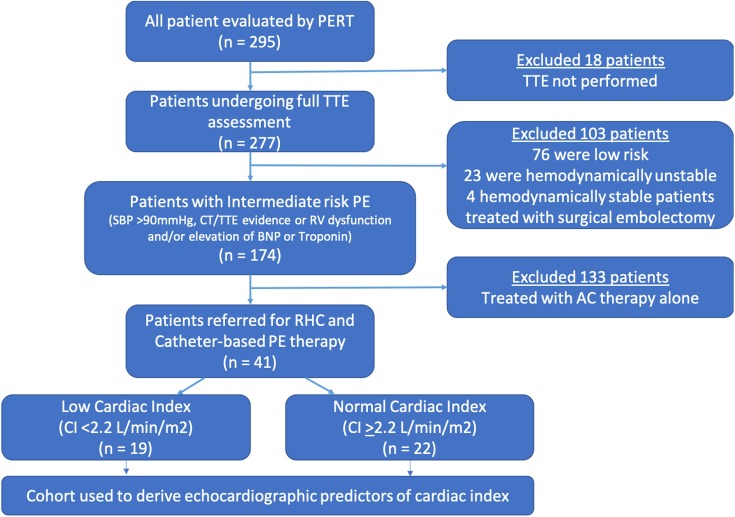
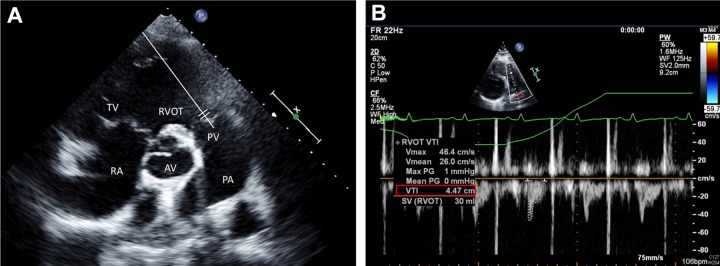
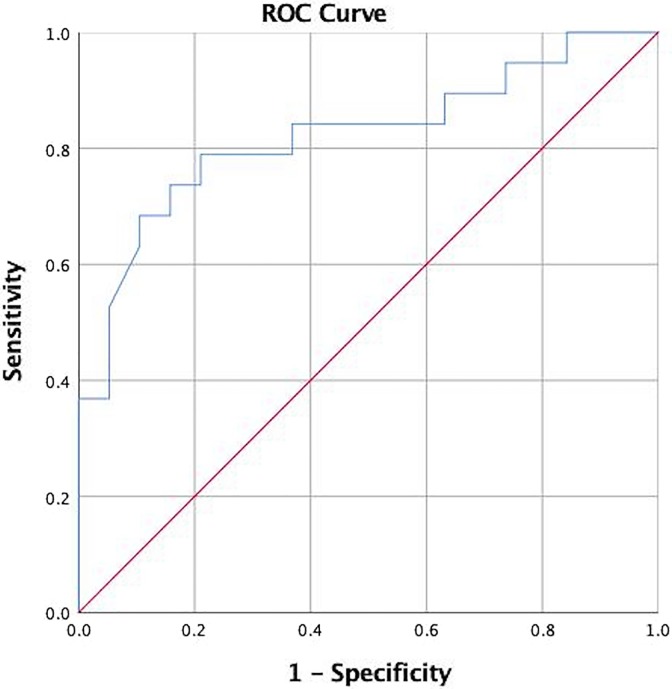
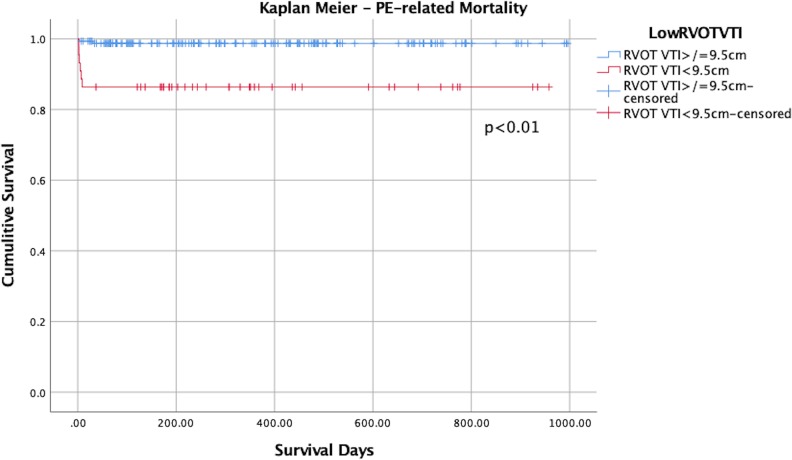
Intermediate-risk pulmonary embolism (PE) has variable outcomes. Current risk stratification models lack the positive predictive value to identify patients at highest risk of PE-related mortality. We identified intermediate-risk PE patients who underwent catheter-based interventions and right heart catheterization (RHC) and identified those with low cardiac index (CI < 2.2 L/min/m2). We utilized regression models to identify echocardiographic predictors of low CI and Kaplan Meier curve to evaluate PE-related mortality when stratified by the echocardiographic predictor. Of 174 intermediate-risk PE patients, 41 underwent RHC. Within this cohort, 46.3% had low CI. Univariable linear regression identified right ventricular outflow tract velocity time integral (RVOT VTI), right/left ventricular ratio, S prime, inferior vena cava diameter, and pulmonary artery systolic pressure as potential predictors of low CI. Multivariable linear regression identified RVOT VTI as significant predictor of low CI (β coefficient 0.124, 95% confidence interval [CI]: 0.01-0.24, P = .034). Right ventricular outflow tract velocity time integral <9.5 cm was associated with increased PE-related mortality, P = .002. A substantial proportion of intermediate-risk PE patients referred for catheter-based interventions had low CI despite normotension. Right ventricular outflow tract velocity time integral was a significant predictor of low CI. Low RVOT VTI was associated with increased PE-related mortality.
Keywords: cardiac index; cardiogenic shock; pulmonary embolism; thrombolysis.
Conflict of interest statement
Figures
References
-
- Konstantinides SV, Torbicki A, Agnelli G, et al. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism: the task force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)endorsed by the European Respiratory Society (ERS). Eur Heart J. 2014;35(43):3033–3069. - PubMed
-
- Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: chest guideline and expert panel report. Chest. 2016;149(2):315–352. doi:10.1016/j.chest.2015.11.026. - PubMed
-
- Secemsky E, Chang Y, Jain CC, et al. Contemporary management and outcomes of patients with massive and submassive pulmonary embolism. Am J Med. 2018;131(12):1506–1514.e0. doi:10.1016/j.amjmed.2018.07.035. - PubMed
-
- Jiménez D, Kopecna D, Tapson V, et al. Derivation and validation of multimarker prognostication for normotensive patients with acute symptomatic pulmonary embolism. Am J Respir Crit Care Med. 2014;189(6):718–726. doi:10.1164/rccm.201311-2040OC. - PubMed
-
- Van Diepen S, Katz JN, Albert NM, et al. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136(16):e232–e268. doi:10.1161/CIR.0000000000000525. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
