

Patient-centered Pharmacist Care in the Hemodialysis Unit: a quasi-experimental interrupted time series study
- PMID: 31722680
- PMCID: PMC6854789
- DOI: 10.1186/s12882-019-1577-6
Patient-centered Pharmacist Care in the Hemodialysis Unit: a quasi-experimental interrupted time series study
Abstract
Background: Nonadherence to medications by patients requiring hemodialysis (HD) leads to unfavorable clinical outcomes. Limited data exist to demonstrate the effect of incorporating patient-centered interventions using concepts of medication therapy management and motivational interview by pharmacists on pharmacoadherence in patients requiring HD. Therefore, we assessed the impact of patient-centered pharmacist care on pharmacoadherence and its outcomes in patients requiring HD.
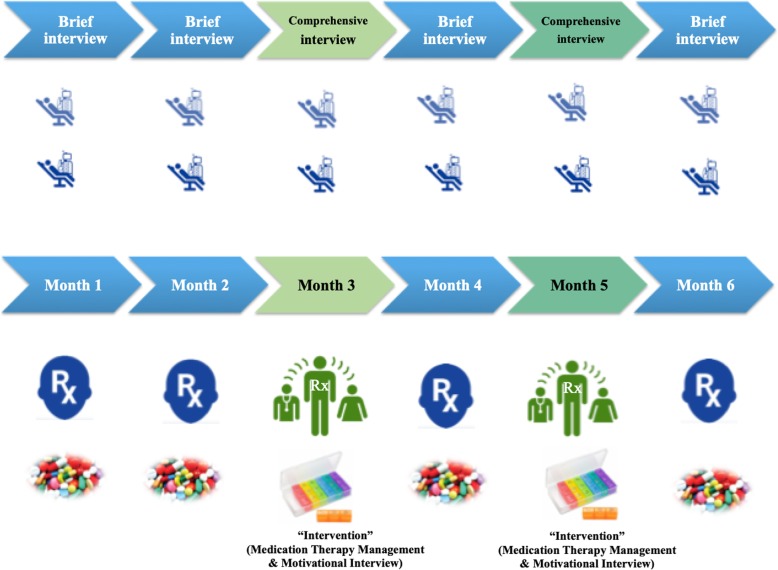
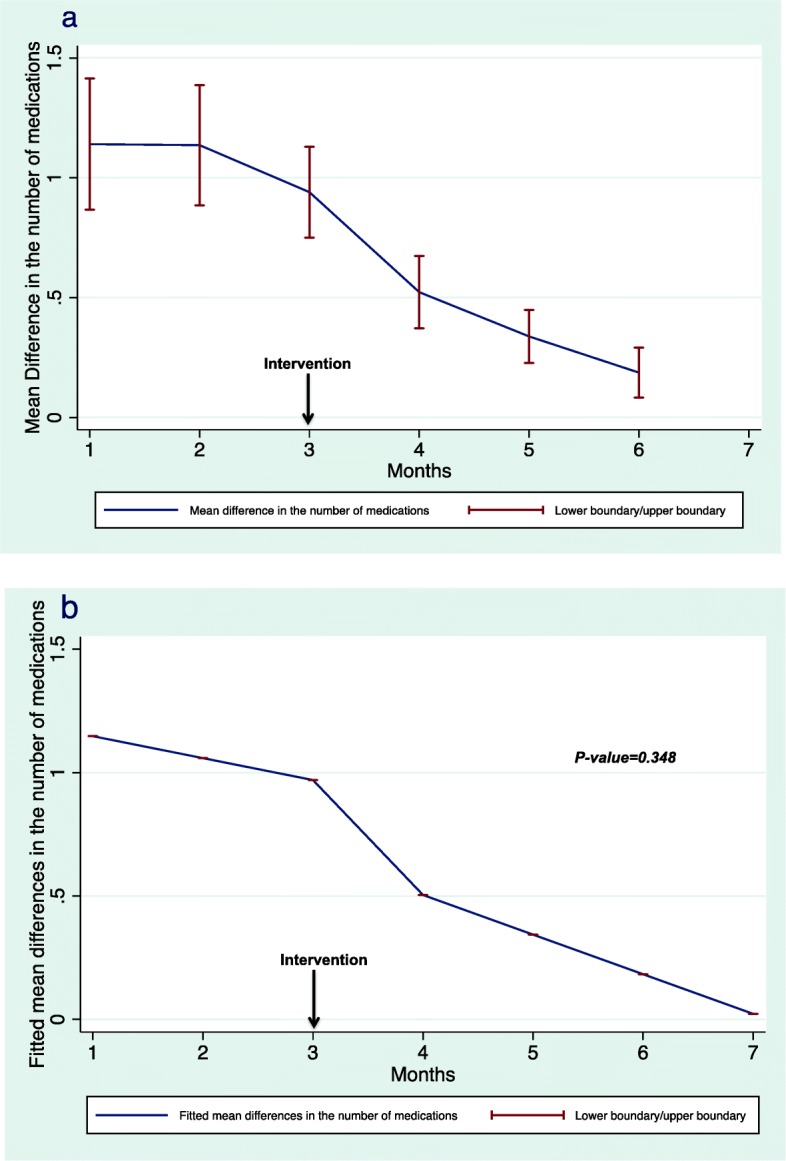
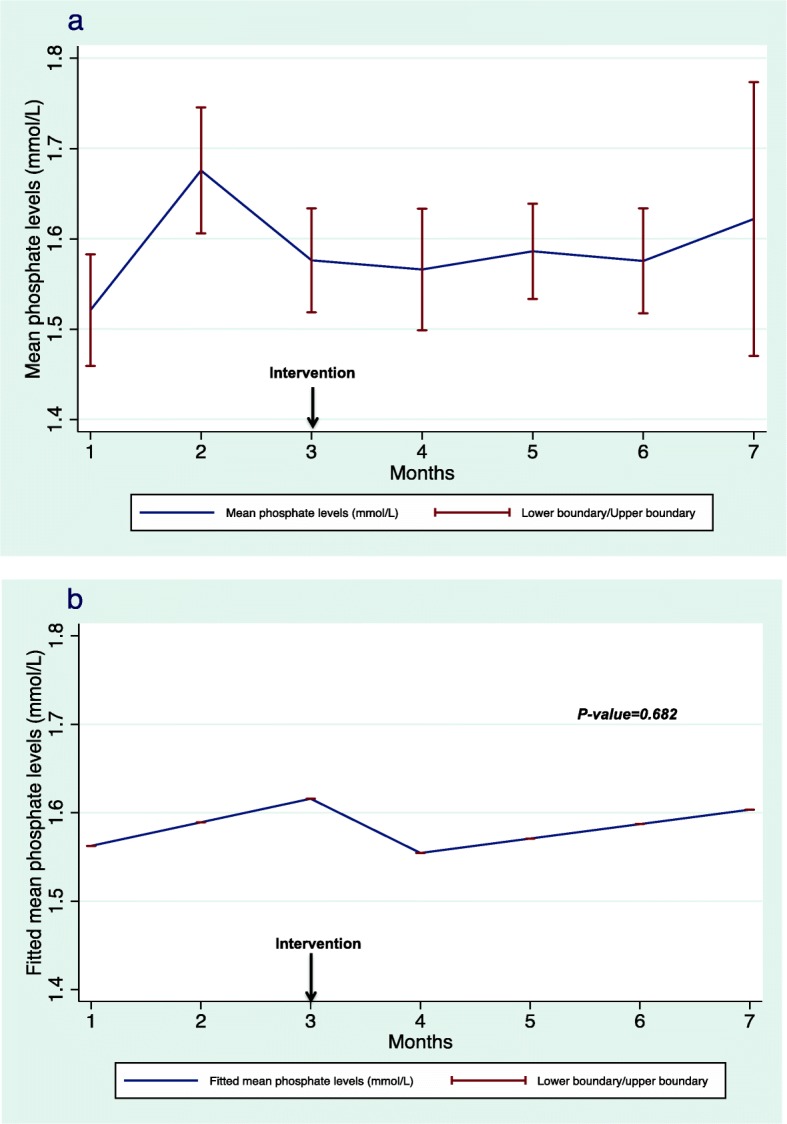
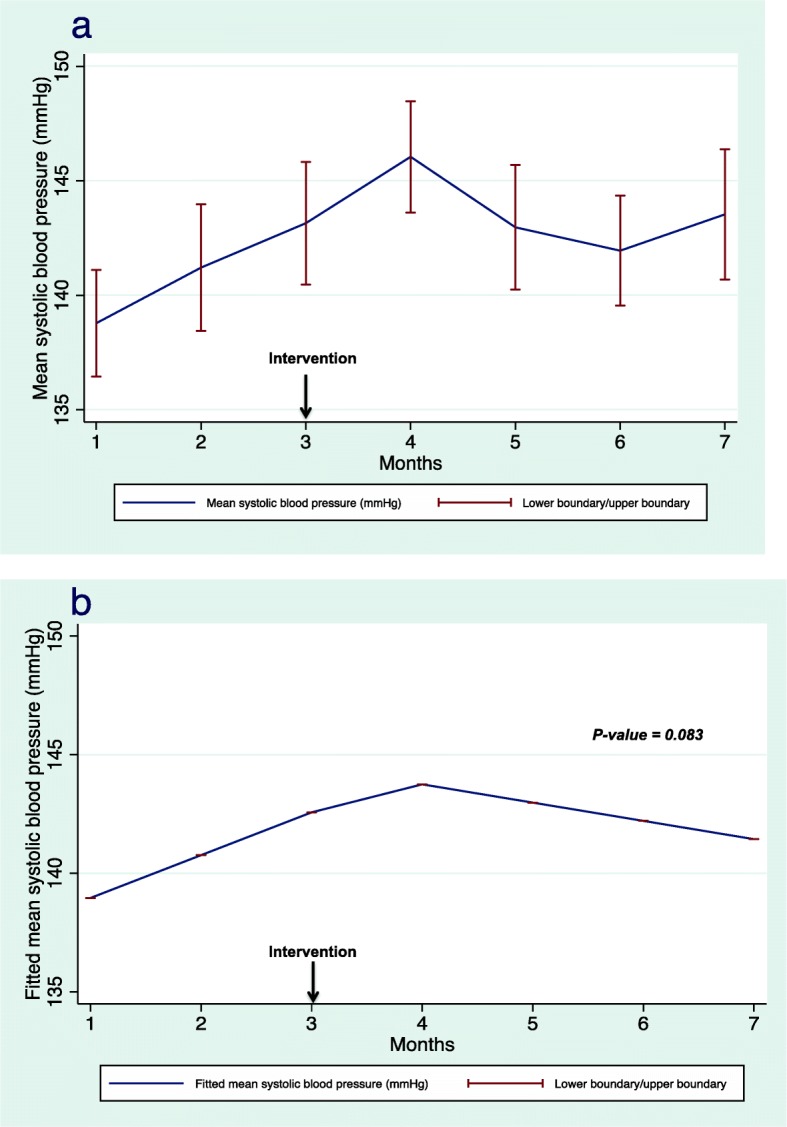
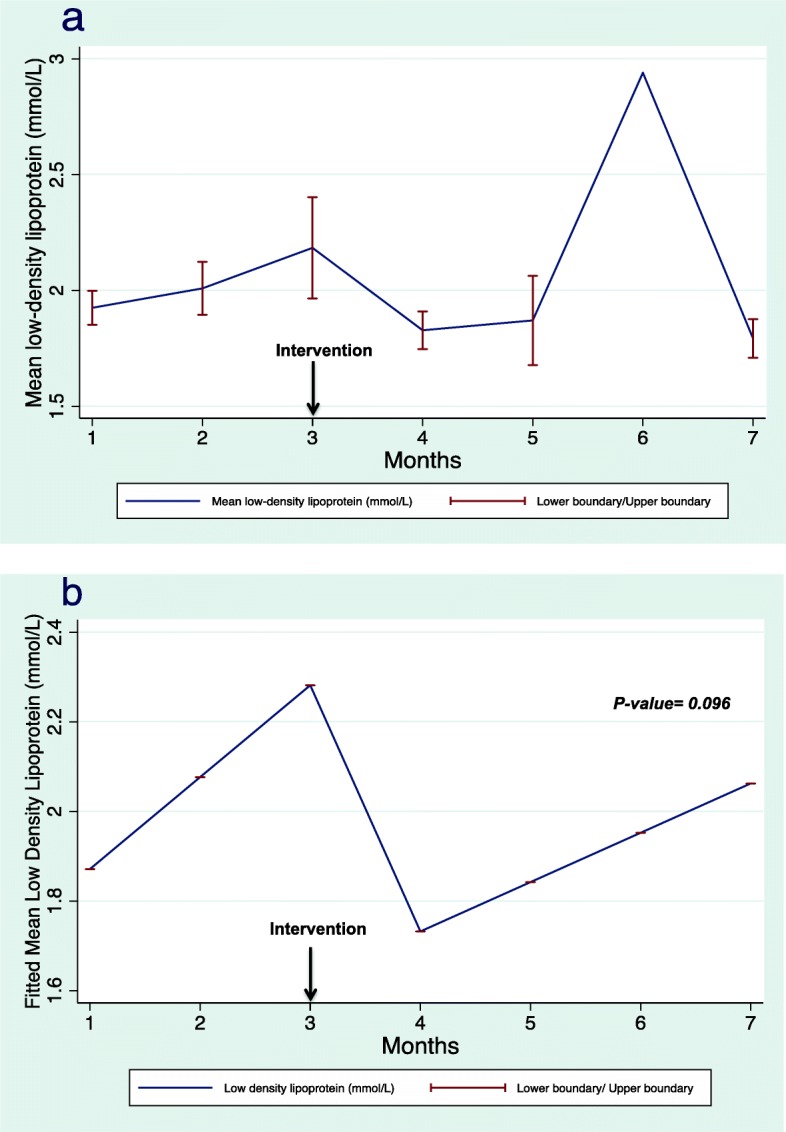
Methods: Adult patients who had received outpatient HD for at least 3 months were enrolled. The study was conducted from October 2016 to April 2017. Pharmacists interviewed the patients at month 1, 2, 4 and 6, and the intervention (comprehensive review) occurred at months 3 and 5. The primary outcome was the change in pharmacoadherence as assessed by pre-HD serum phosphate levels and the differences in the number of medications between patient' self-report and medications records at the electronic healthcare records (EHRs). The secondary outcomes included changes in systolic blood pressure (SBP), glycosylated hemoglobin levels, serum low-density lipoprotein (LDL) levels, and the prevalence and types of medication-related problems (MRPs).
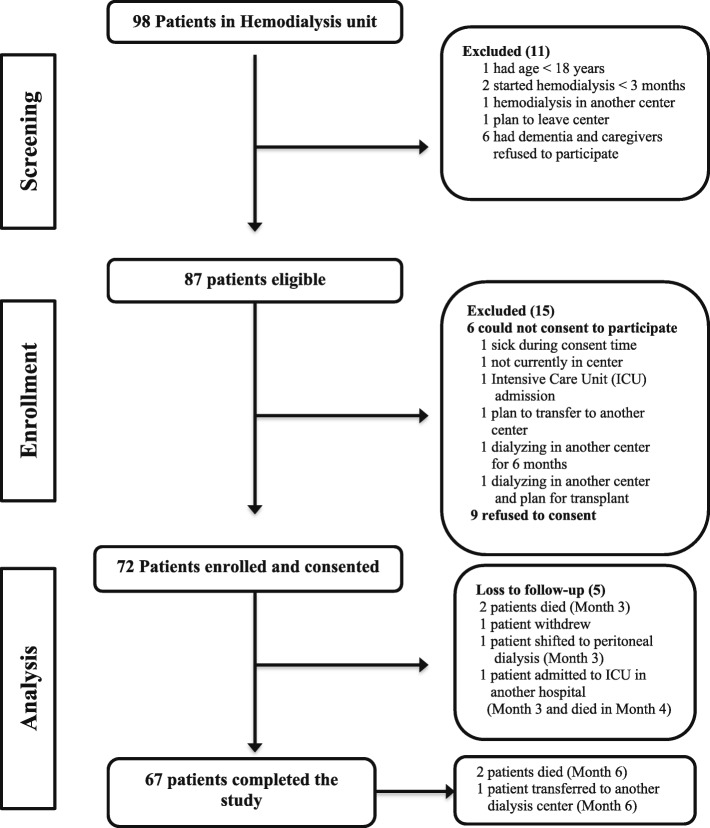
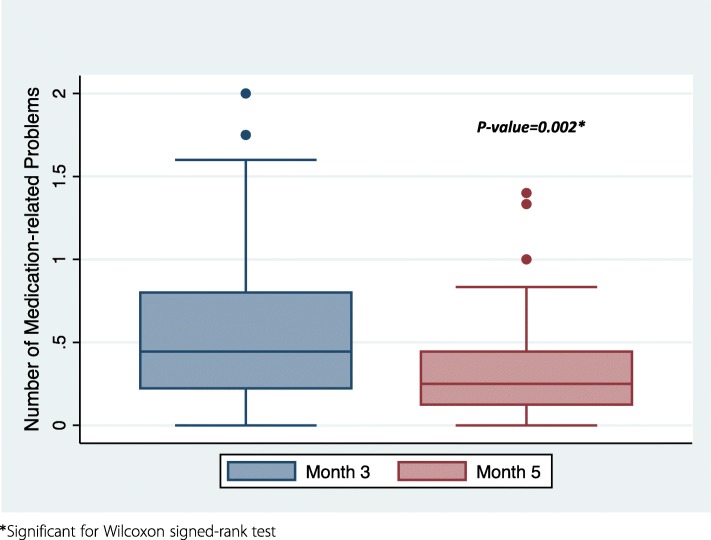
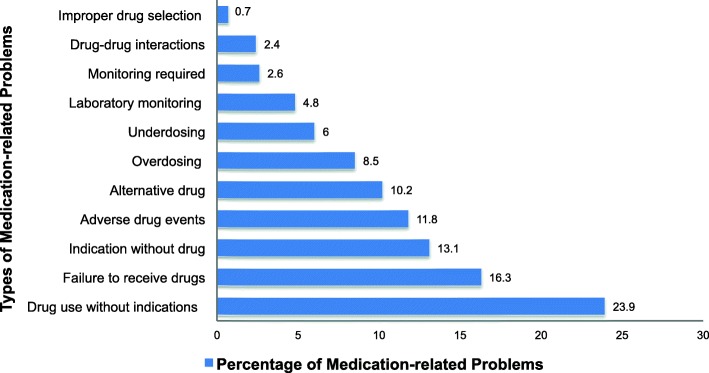
Results: Seventy-two patients were enrolled. Their median age was 59 (interquartile range: 47-67.5) years, and 53% were men. Pre- and post-intervention pharmacoadherence, as indicated by serum phosphate levels and the differences in the number of medications between patient' self-report and the medication records at the EHRs, did not significantly differ (p = 0.682 and 0.348, respectively). Mean SBP and mean LDL did not significantly change post-intervention. The median number of MRPs declined between Months 3 and 5 (p = 0.002): the prevalence of MRPs at Month 3 was 44.9% (95 confidence interval [CI]: 40.4-49.3) and decreased to 29.8% (95 CI: 25.6-34.3) at Month 5. Drug use without indication was the most frequent MRP (23.9%).
Conclusions: Patient-centered pharmacist care did not result in significant changes in pharmacoadherence. However, its clinical utility as a tool to identify and mitigate MRPs in patients requiring HD is indisputable.
Trial registration: ClinicalTrials.gov identifier: NCT03576404 (retrospectively registered on July 3rd, 2018).
Keywords: Adherence; Hemodialysis; Medication therapy management; Medication-related problems; Motivational interview; Patient-centered pharmacist care; Pharmacoadherence.
Conflict of interest statement
None to declare.
Figures
References
-
- World Health Organization. Adherence to long-term therapies. Evidence for action. 2003.http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf?.... Accessed 28 March 2016.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
