

Variation in post-colonoscopy colorectal cancer across colonoscopy providers in English National Health Service: population based cohort study
- PMID: 31722875
- PMCID: PMC6849511
- DOI: 10.1136/bmj.l6090
Variation in post-colonoscopy colorectal cancer across colonoscopy providers in English National Health Service: population based cohort study
Abstract
Objectives: To quantify post-colonoscopy colorectal cancer (PCCRC) rates in England by using recent World Endoscopy Organisation guidelines, compare incidence among colonoscopy providers, and explore associated factors that could benefit from quality improvement initiatives.
Design: Population based cohort study.
Setting: National Health Service in England between 2005 and 2013.
Population: All people undergoing colonoscopy and subsequently diagnosed as having colorectal cancer up to three years after their investigation (PCCRC-3yr).
Main outcome measures: National trends in incidence of PCCRC (within 6-36 months of colonoscopy), univariable and multivariable analyses to explore factors associated with occurrence, and funnel plots to measure variation among providers.
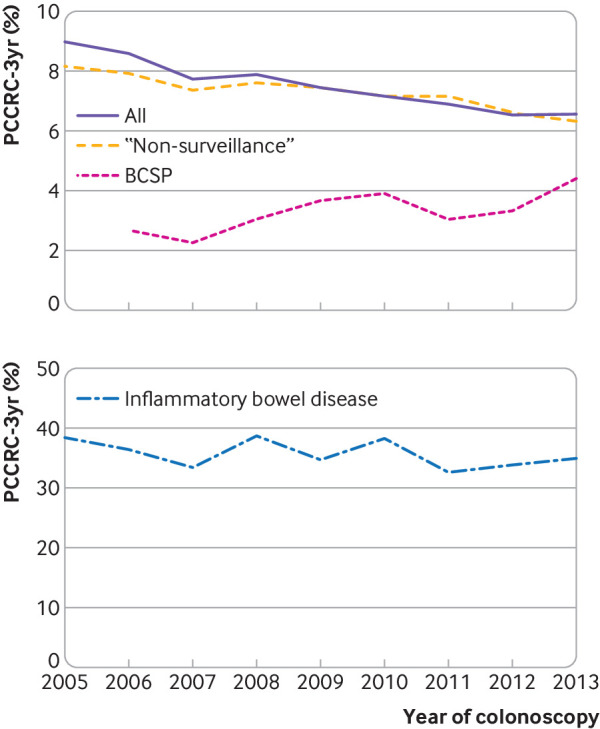
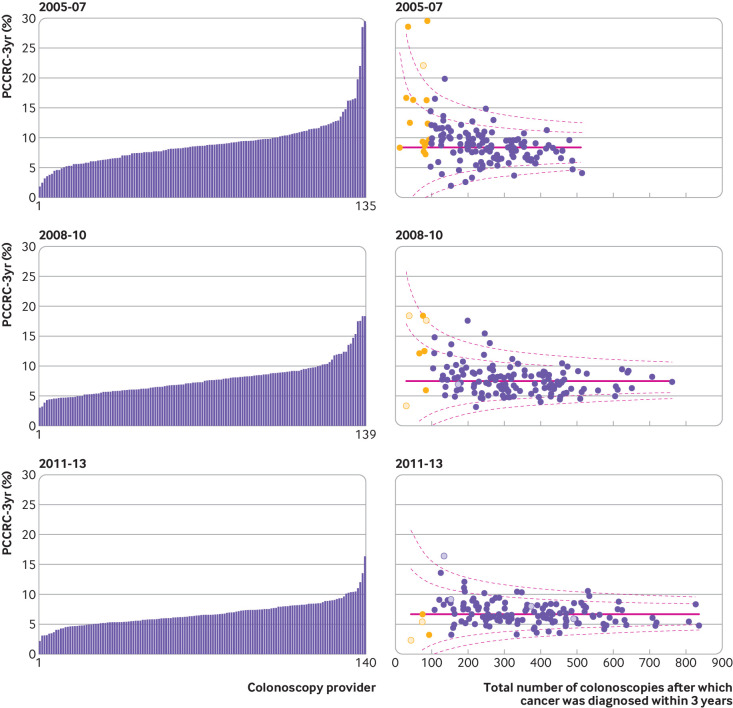
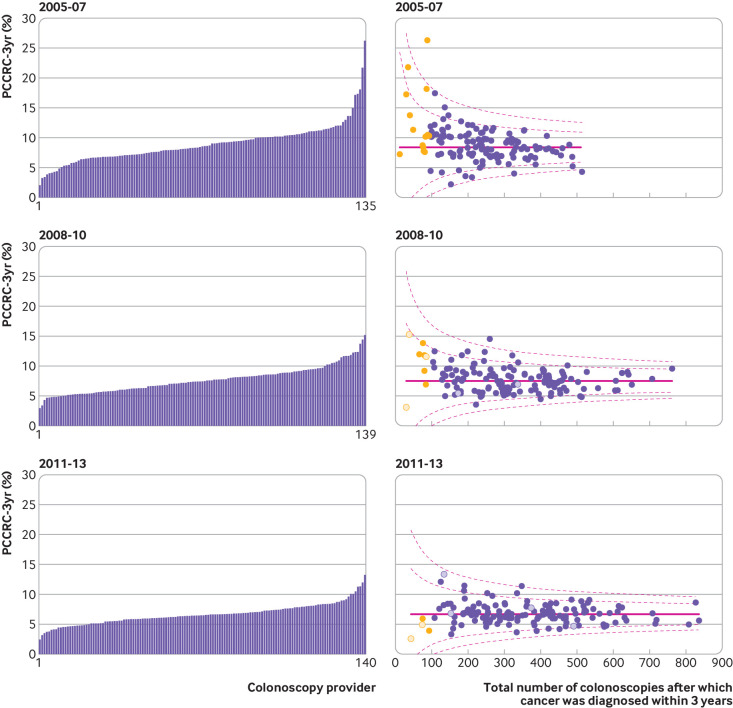
Results: The overall unadjusted PCCRC-3yr rate was 7.4% (9317/126 152), which decreased from 9.0% in 2005 to 6.5% in 2013 (P<0.01). Rates were lower for colonoscopies performed under the NHS bowel cancer screening programme (593/16 640, 3.6%), while they were higher for those conducted by non-NHS providers (187/2009, 9.3%). Rates were higher in women, in older age groups, and in people with inflammatory bowel disease or diverticular disease, in those with higher comorbidity scores, and in people with previous cancers. Substantial variation in rates among colonoscopy providers remained after adjustment for case mix.
Conclusions: Wide variation exists in PCCRC-3yr rates across NHS colonoscopy providers in England. The lowest incidence was seen in colonoscopies performed under the NHS bowel cancer screening programme. Quality improvement initiatives are needed to address this variation in rates and prevent colorectal cancer by enabling earlier diagnosis, removing premalignant polyps, and therefore improving outcomes.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Bobby Moore Fund, Cancer Research UK, Yorkshire Cancer Research, and Crohn’s and Colitis UK for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Unacceptable variation in screening colonoscopy.BMJ. 2019 Nov 13;367:l6384. doi: 10.1136/bmj.l6384. BMJ. 2019. PMID: 31722874 No abstract available.
-
Post-colonoscopy colorectal cancer: patients can be reassured that UK endoscopy is already engaged in quality assessment and continual improvement.BMJ. 2019 Dec 10;367:l6910. doi: 10.1136/bmj.l6910. BMJ. 2019. PMID: 31822486 No abstract available.
References
-
- Cancer Research UK. Bowel Cancer Statistics 2016. Accessed 01/02/2019. https://www.cancerresearchuk.org/health-professional/cancer-statistics/s....
-
- Morris EJA, Rutter MD, Finan PJ, Thomas JD, Valori R. Post-colonoscopy colorectal cancer (PCCRC) rates vary considerably depending on the method used to calculate them: a retrospective observational population-based study of PCCRC in the English National Health Service. Gut 2015;64:1248-56. 10.1136/gutjnl-2014-308362. - DOI - PMC - PubMed
-
- Rees CJ, Thomas Gibson S, Rutter MD, et al. British Society of Gastroenterology, the Joint Advisory Group on GI Endoscopy, the Association of Coloproctology of Great Britain and Ireland UK key performance indicators and quality assurance standards for colonoscopy. Gut 2016;65:1923-9. 10.1136/gutjnl-2016-312044. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical