

A view on drug resistance in cancer
- PMID: 31723286
- PMCID: PMC8008476
- DOI: 10.1038/s41586-019-1730-1
A view on drug resistance in cancer
Abstract
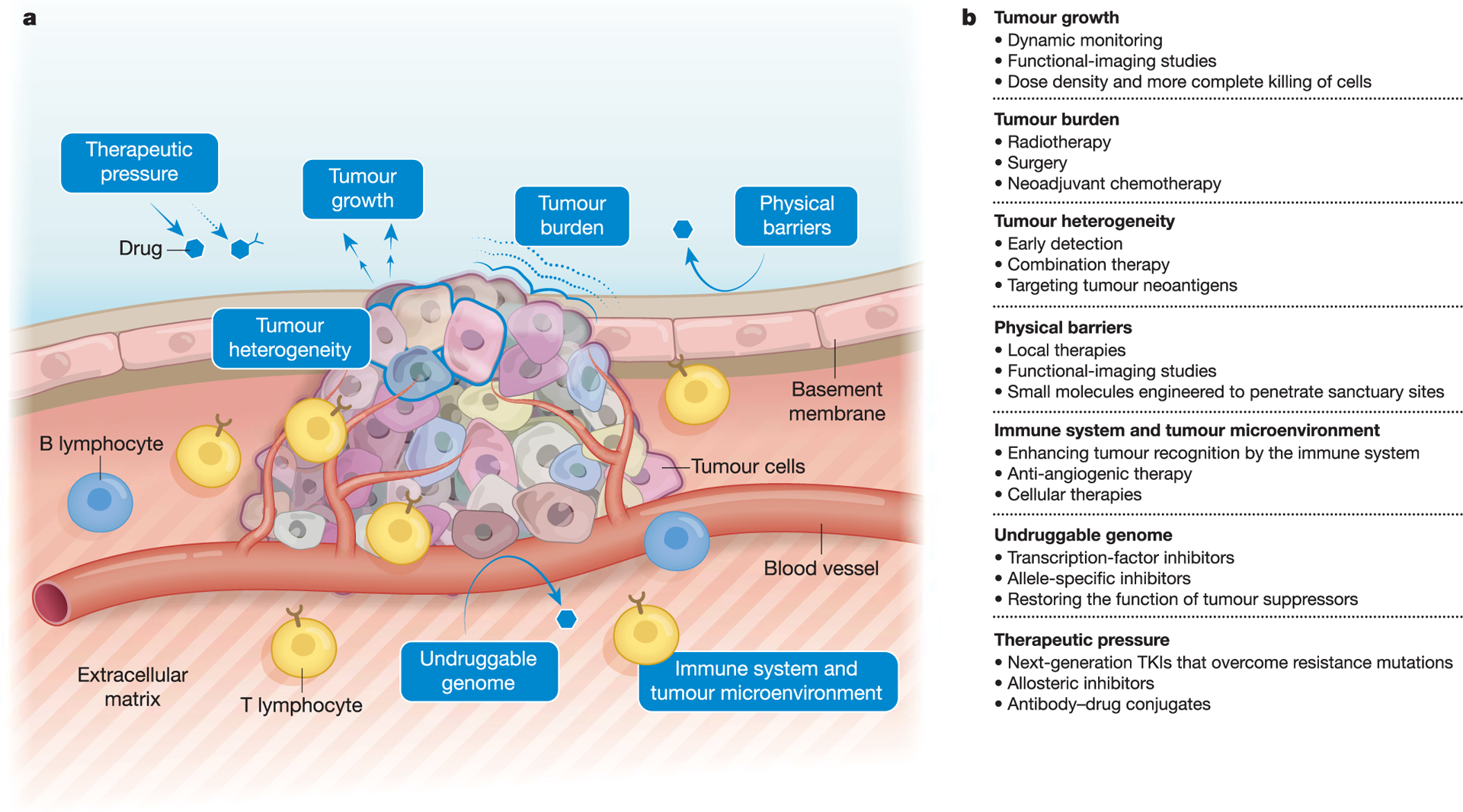
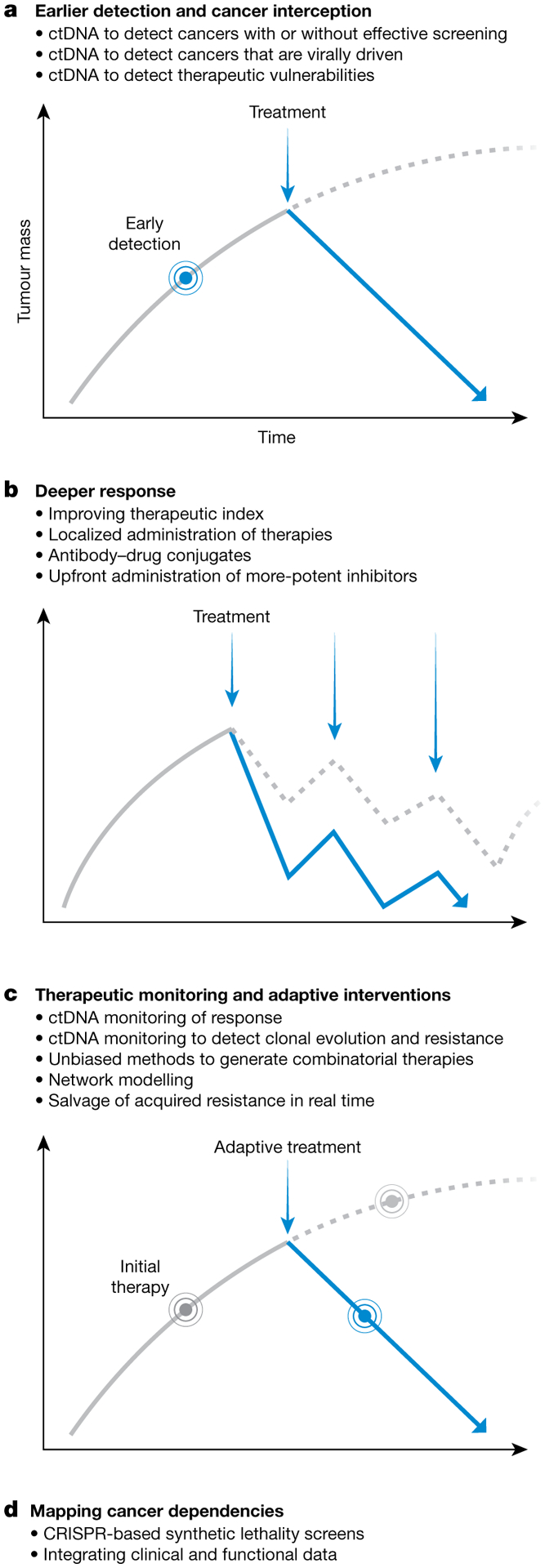
The problem of resistance to therapy in cancer is multifaceted. Here we take a reductionist approach to define and separate the key determinants of drug resistance, which include tumour burden and growth kinetics; tumour heterogeneity; physical barriers; the immune system and the microenvironment; undruggable cancer drivers; and the many consequences of applying therapeutic pressures. We propose four general solutions to drug resistance that are based on earlier detection of tumours permitting cancer interception; adaptive monitoring during therapy; the addition of novel drugs and improved pharmacological principles that result in deeper responses; and the identification of cancer cell dependencies by high-throughput synthetic lethality screens, integration of clinico-genomic data and computational modelling. These different approaches could eventually be synthesized for each tumour at any decision point and used to inform the choice of therapy.
Conflict of interest statement
Figures
References
-
- Goodman LS et al. Nitrogen mustard therapy; use of methyl-bis (beta-chloroethyl) amine hydrochloride and tris (beta-chloroethyl) amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. J. Am. Med. Assoc 132, 126–132 (1946). - PubMed
-
This study and the next one (reference 2) were the first clinical reports of chemotherapy in advanced cancers.
-
- Farber S & Diamond LK Temporary remissions in acute leukemia in children produced by folic acid antagonist, 4-aminopteroyl-glutamic acid. N. Engl. J. Med 238, 787–793 (1948). - PubMed
-
- DeVita VT Jr et al. Curability of advanced Hodgkin’s disease with chemotherapy. Long-term follow-up of MOPP-treated patients at the National Cancer Institute. Ann. Intern. Med 92, 587–595 (1980). - PubMed
-
This study and the next one (reference 5) were the first clinical trials of combination chemotherapy, in advanced Hodgkin’s lymphoma and localized breast cancer, respectively.
-
- Bonadonna G et al. Combination chemotherapy as an adjuvant treatment in operable breast cancer. N. Engl. J. Med 294, 405–410 (1976). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
