

Immune checkpoint inhibitor-associated gastrointestinal and hepatic adverse events and their management
- PMID: 31723355
- PMCID: PMC6831976
- DOI: 10.1177/1756284819884196
Immune checkpoint inhibitor-associated gastrointestinal and hepatic adverse events and their management
Abstract
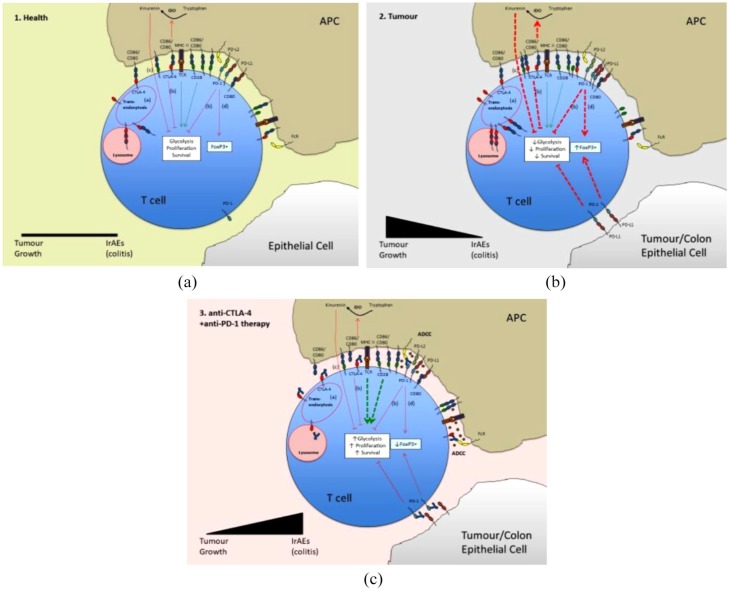
Background: Drug-induced colitis is a known complication of therapies that alter the immune balance, damage the intestinal barrier or disturb intestinal microbiota. Immune checkpoint inhibitors (ICI) directed against cancer cells may result in activated T lymphocyte-induced immune-related adverse events (AEs), including immune-related colitis and hepatitis. The aim of this review article is to summarize the incidence of gastrointestinal (GI) and hepatic AEs related to ICI therapy. We have also looked at the pathogenesis of immune-mediated AEs and propose management strategies based on current available evidence.
Methods: A literature search using PubMed and Medline databases was undertaken using relevant search terms pertaining to names of individual drugs, mechanism of action, related AEs and their management.
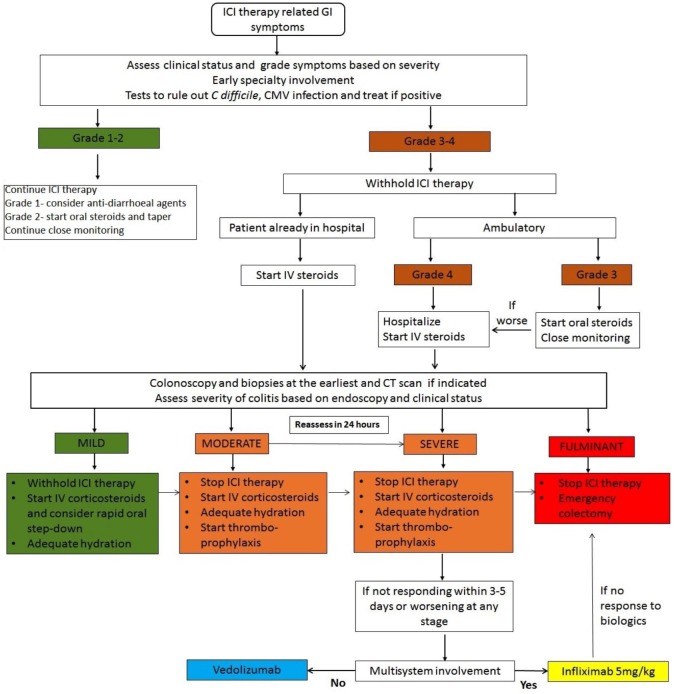
Results: ICI-related GI AEs are common, and colitis appears to be the most common side effect, with some studies reporting incidence as high as 30%. The incidence of both all-grade colitis and hepatitis were highest with combination therapy with anti-CTLA-4/PD-1; severity of colitis was dose-dependent (anti-CTLA-4). Early intervention is associated with better outcomes.
Conclusion: ICI-related GI and hepatic AEs are common and clinicians need to be aware. Patients with GI AEs benefit from early diagnosis using endoscopy and computed tomography. Early intervention with oral steroids is effective in the majority of patients, and in steroid-refractory colitis infliximab and vedolizumab have been reported to be useful; mycophenolate has been used for steroid-refractory hepatitis.
Keywords: anti-CTLA-4; anti-PD1; anti-PDL1; immune checkpoint inhibitors; immune-related colitis; immune-related hepatitis; management.
© The Author(s), 2019.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Michot JM, Bigenwald C, Champiat S, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer 2016; 54: 139–148. - PubMed
-
- National Institute of Health. Common Terminology Criteria for Adverse Events (CTCAE). NIH Publ. 2010;2009:0–71.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
