

Miliary tuberculosis: A new look at an old foe
- PMID: 31723681
- PMCID: PMC6850233
- DOI: 10.1016/j.jctube.2016.03.003
Miliary tuberculosis: A new look at an old foe
Abstract
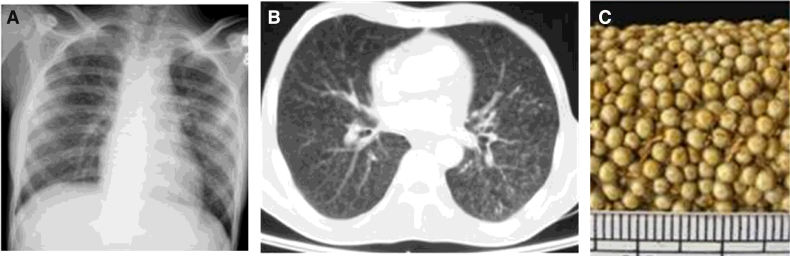
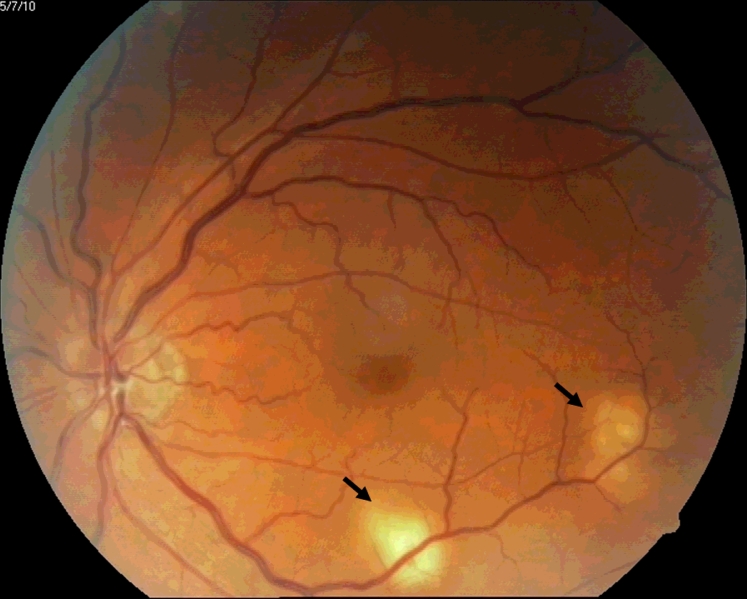
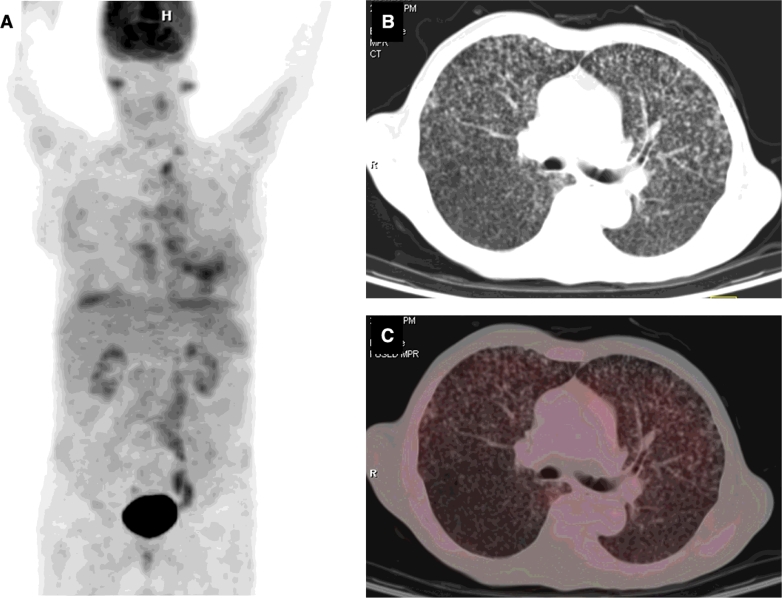
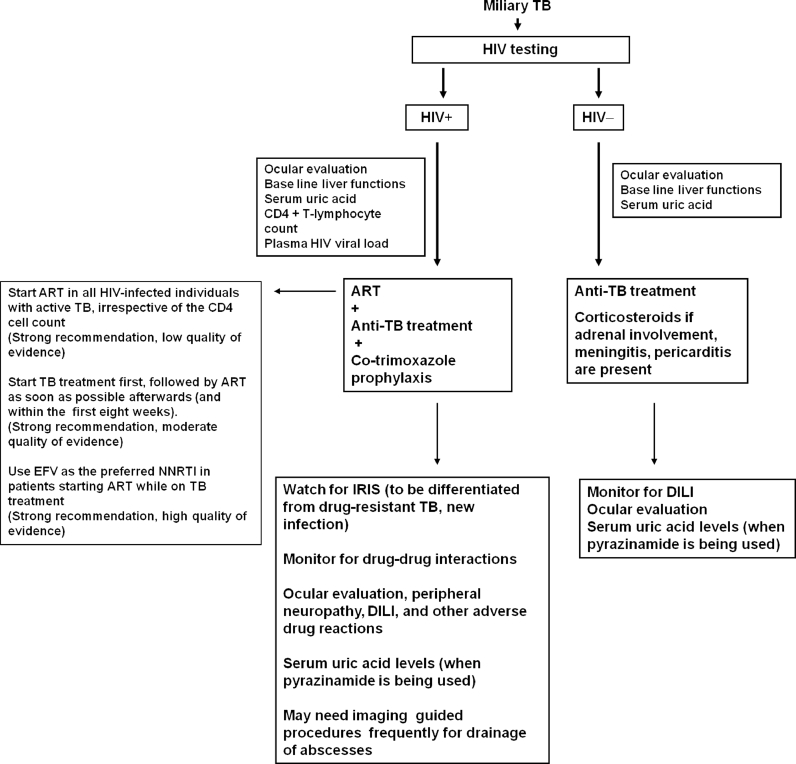
Miliary tuberculosis (TB), is a fatal form of disseminated TB characterized by tiny tubercles evident on gross pathology similar to innumerable millet seeds in size and appearance. Global HIV/AIDS pandemic and increasing use of immunosuppressive drugs have altered the epidemiology of miliary TB. Keeping in mind its protean manifestations, clinicians should have a low threshold for suspecting miliary TB. Careful physical examination should focus on identifying organ system involvement early, particularly TB meningitis, as this has therapeutic significance. Fundus examination for detecting choroid tubercles can help in early diagnosis as their presence is pathognomonic of miliary TB. Imaging modalities help in recognizing the miliary pattern, define the extent of organ system involvement and facilitate image guided fine-needle aspiration cytology or biopsy from various organ sites. Sputum or BAL fluid examination, pleural, pericardial, peritoneal fluid and cerebrospinal fluid studies, fine needle aspiration cytology or biopsy of the lymph nodes, needle biopsy of the liver, bone marrow aspiration and biopsy, testing of body fluids must be carried out. GeneXpert MTB/RIF, line probe assay, mycobacterial culture and drug-susceptibility testing must be carried out as appropriate and feasible. Treatment of miliary TB should be started at the earliest as this can be life saving. Response to first-line anti-TB drugs is good. Screening and monitoring for complications like acute respiratory distress syndrome (ARDS), adverse drug reactions like drug-induced liver injury, drug-drug interactions, especially in patients co-infected with HIV/AIDS, are warranted. Sparse data are available from randomized controlled trials regarding optimum regimen and duration of anti-TB treatment.
Keywords: Complications; Diagnosis; Human immunodeficiency virus; Miliary tuberculosis; Treatment.
© 2016 Published by Elsevier Ltd.
Figures

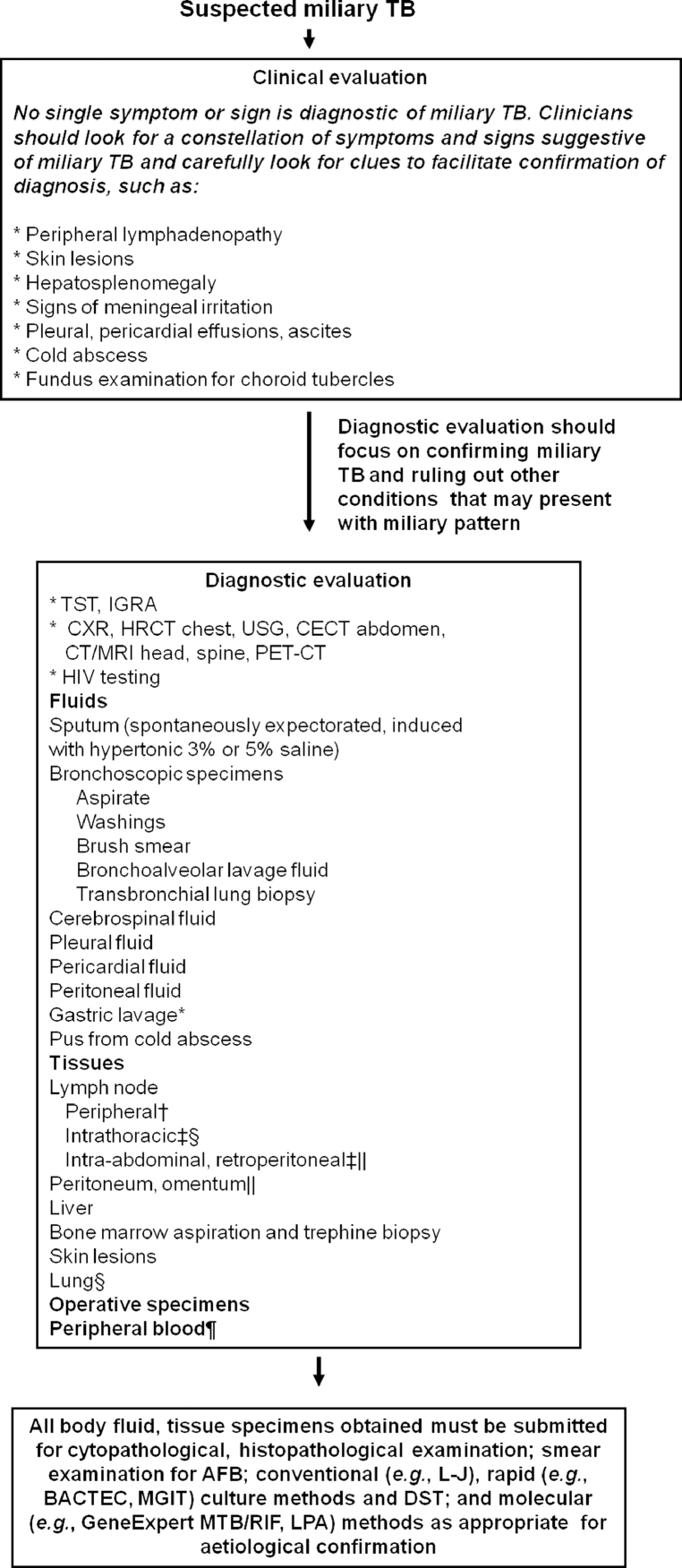
 Useful in advanced HIV infection. TB = tuberculosis; TST = tuberculin skin test; IGRA = interferon-γ release assays; HRCT = high resolution computed tomography; CECT = contrast enhanced computed tomography; MRI = magnetic resonance imaging; FNAC = fine needle aspiration cytology; HIV = human immunodeficiency virus; AFB = acid-fast bacilli; L–J = Lowenstein–Jensen medium; DST = drug-susceptibility testing; MGIT = mycobacterial growth inhibitor tube; BACTEC = radiometric culture method; PCR = polymerase chain reaction; GeneExpert MTB/RIF = GeneXpert MTB/RIF assay (Cepheid, Sunnyvale, CA); LPA = line probe assay Adapted and reproduced with permission from Sharma et al. .
Useful in advanced HIV infection. TB = tuberculosis; TST = tuberculin skin test; IGRA = interferon-γ release assays; HRCT = high resolution computed tomography; CECT = contrast enhanced computed tomography; MRI = magnetic resonance imaging; FNAC = fine needle aspiration cytology; HIV = human immunodeficiency virus; AFB = acid-fast bacilli; L–J = Lowenstein–Jensen medium; DST = drug-susceptibility testing; MGIT = mycobacterial growth inhibitor tube; BACTEC = radiometric culture method; PCR = polymerase chain reaction; GeneExpert MTB/RIF = GeneXpert MTB/RIF assay (Cepheid, Sunnyvale, CA); LPA = line probe assay Adapted and reproduced with permission from Sharma et al. .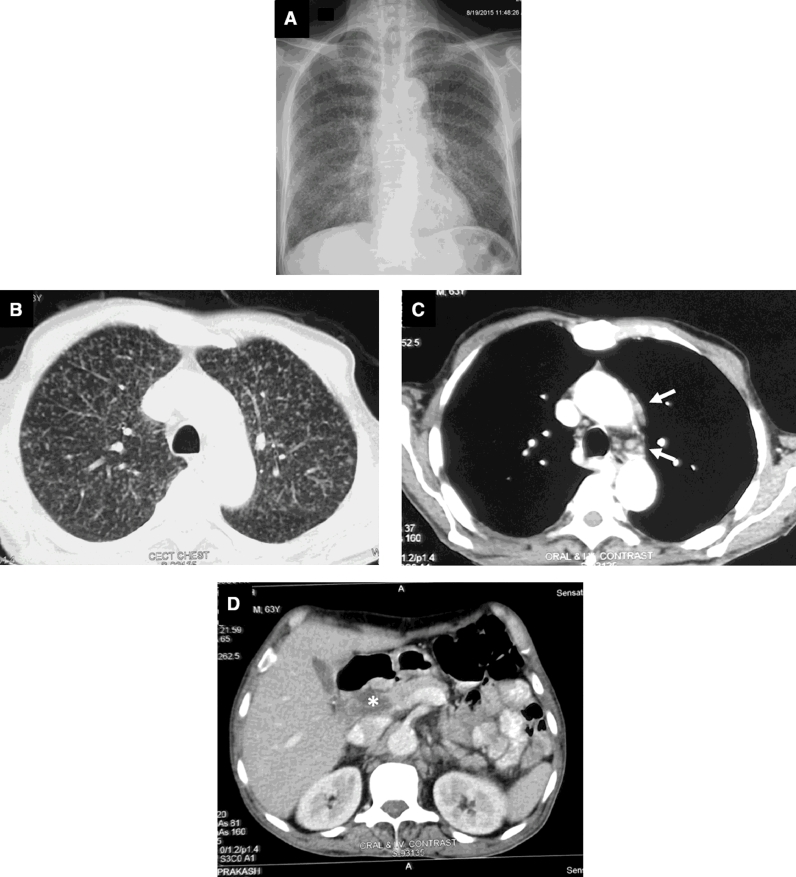
References
-
- Global tuberculosis control. WHO report 2015. WHO/HTM/ TB/2015.22. Geneva: World Health Organization; 2015.
-
- Sharma S.K., Mohan A., Schlossberg D. Tuberculosis and nontuberculous mycobacterial infections. 6th ed. American Society for Microbiology Press; Washington: 2011. Miliary tuberculosis; pp. 415–435.
-
- Sharma S.K., Mohan A. Disseminated and miliary tuberculosis. In: Sharma SK, Mohan A, editors. Tuberculosis. 2nd ed. Jaypee Brothers Medical Publishers; New Delhi: 2009. pp. 493–518.
-
- Sharma S.K., Mohan A., Sharma A., Mitra D.K. Miliary tuberculosis: new insights into an old disease. Lancet Infect Dis. 2005;5:415–430. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
