

Orbital and external ocular manifestations of Mycobacterium tuberculosis: A review of the literature
- PMID: 31723688
- PMCID: PMC6850259
- DOI: 10.1016/j.jctube.2015.11.001
Orbital and external ocular manifestations of Mycobacterium tuberculosis: A review of the literature
Abstract
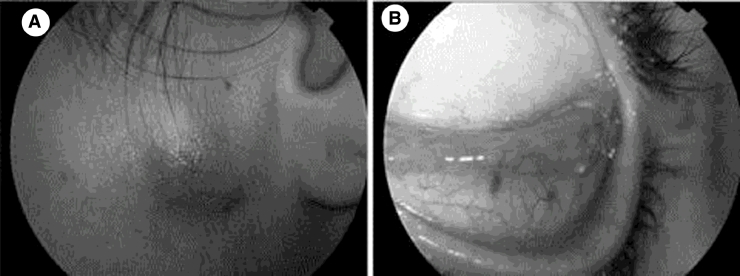
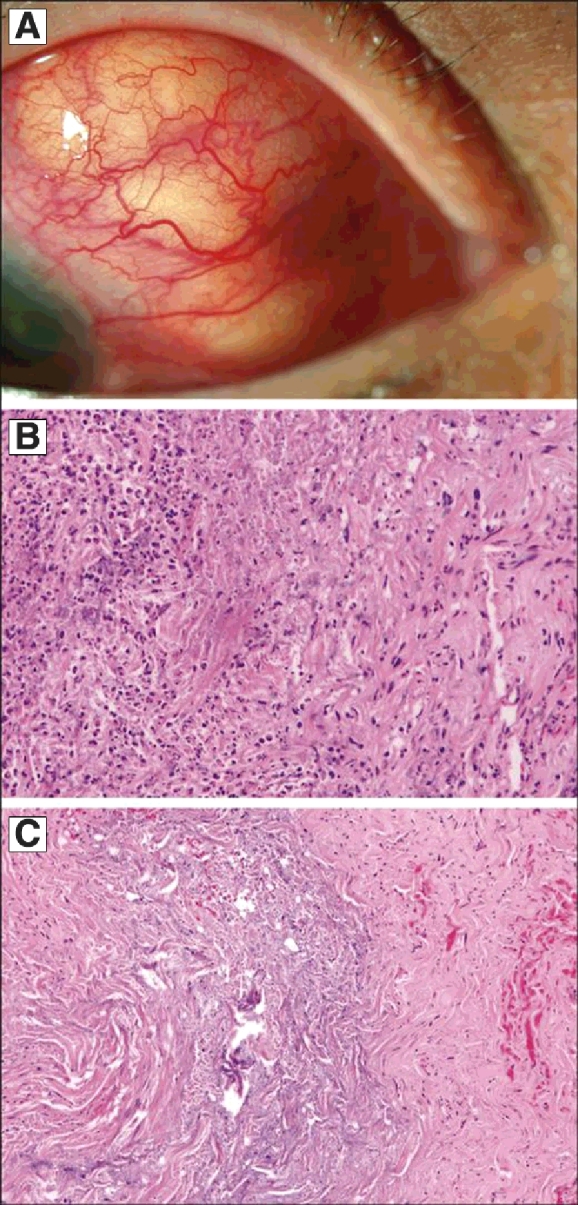
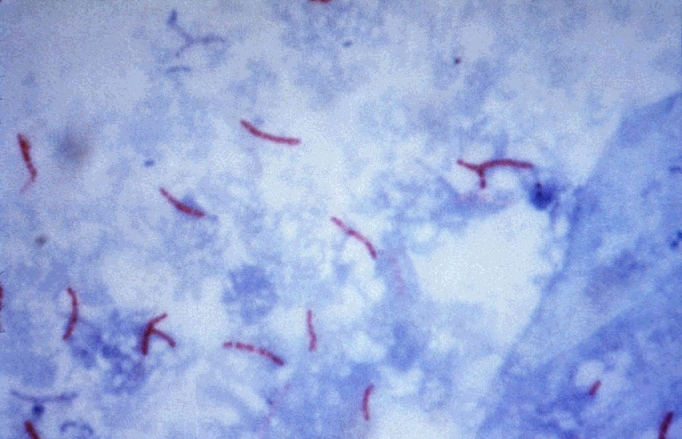
Tuberculosis (TB) is an airborne infectious disease caused by Mycobacterium tuberculosis that most commonly affects the lungs. However, extrapulmonary manifestations of TB can affect the eye and surrounding orbital tissues. TB can affect nearly any tissue in the eye, and a high index of suspicion is required for accurate diagnosis. Systemic anti-tuberculosis treatment is required in cases of ocular TB, and steroids are sometimes necessary to prevent tissue damage secondary to inflammation. Delays in diagnosis are common and can result in morbidities such as loss of an affected eye. It is important for ophthalmologists and infectious disease specialists to work together to accurately diagnose and treat ocular TB in order to prevent vision loss. This article reports the various known presentations of orbital and external ocular TB and reviews important elements of diagnosis and treatment.
Keywords: Eye; Mycobacterium; Ocular; Orbit; Tuberculosis.
© 2016 The Authors.
Figures



Similar articles
-
Intraocular manifestations of mycobacterium tuberculosis: A review of the literature.J Clin Tuberc Other Mycobact Dis. 2017 Feb 17;7:13-21. doi: 10.1016/j.jctube.2017.01.003. eCollection 2017 May. J Clin Tuberc Other Mycobact Dis. 2017. PMID: 31723696 Free PMC article. Review.
-
Characterization of and advanced diagnostic methods for ocular tuberculosis and tuberculosis.Int J Ophthalmol. 2020 Nov 18;13(11):1820-1826. doi: 10.18240/ijo.2020.11.21. eCollection 2020. Int J Ophthalmol. 2020. PMID: 33215016 Free PMC article. Review.
-
Ocular Tuberculosis Without a Lung Primary.Cureus. 2020 May 1;12(5):e7920. doi: 10.7759/cureus.7920. Cureus. 2020. PMID: 32494534 Free PMC article.
-
Tuberculosis and the eye.Niger J Clin Pract. 2006 Jun;9(1):68-76. Niger J Clin Pract. 2006. PMID: 16986294 Review.
-
Mycobacterium-related ocular inflammatory disease: diagnosis and management.Ann Acad Med Singap. 2006 Mar;35(3):203-9. Ann Acad Med Singap. 2006. PMID: 16625271
Cited by
-
Tubercular Episcleritis: A Review of Literature.Middle East Afr J Ophthalmol. 2022 Nov 23;29(1):51-55. doi: 10.4103/meajo.meajo_315_21. eCollection 2022 Jan-Mar. Middle East Afr J Ophthalmol. 2022. PMID: 36685347 Free PMC article. Review.
-
ORBITAL CELLULITIS IN PULMONARY TUBERCULOSIS: A CASE REPORT.Afr J Infect Dis. 2020 Jul 31;14(2):48-52. doi: 10.21010/ajid.v14i2.8. eCollection 2020. Afr J Infect Dis. 2020. PMID: 33884351 Free PMC article.
-
Whipple's disease scleral nodules: a novel presentation in 2 consecutive patients.BMC Ophthalmol. 2020 Oct 16;20(1):413. doi: 10.1186/s12886-020-01695-4. BMC Ophthalmol. 2020. PMID: 33066757 Free PMC article.
-
Case Report: Unveiling the Unseen - Ocular Tuberculosis Presenting as Chalazion.Am J Trop Med Hyg. 2024 Aug 13;111(4):841-843. doi: 10.4269/ajtmh.24-0271. Print 2024 Oct 2. Am J Trop Med Hyg. 2024. PMID: 39137753 Free PMC article.
-
Intraocular manifestations of mycobacterium tuberculosis: A review of the literature.J Clin Tuberc Other Mycobact Dis. 2017 Feb 17;7:13-21. doi: 10.1016/j.jctube.2017.01.003. eCollection 2017 May. J Clin Tuberc Other Mycobact Dis. 2017. PMID: 31723696 Free PMC article. Review.
References
-
- Tabbara K. Tuberculosis. Curr Opin Ophthalmol. 2007;18(6):493–501. - PubMed
-
- Jones R.M., Brosseau L.M. Aerosol transmission of infectious disease. J Occup Environ Med. 2015;57(5):501–508. - PubMed
-
- Sanches I., Carvalho A., Duarte R. Who are the patients with extrapulmonary tuberculosis? Rev Port Pneumol. 2014;21(2):90–93. - PubMed
-
- Gupta V., Gupta A., Rao N.A. Intraocular tuberculosis – an update. Surv Ophthalmol. 2007;52(6):561–587. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
