

Histopathologic review of granulomatous inflammation
- PMID: 31723695
- PMCID: PMC6850266
- DOI: 10.1016/j.jctube.2017.02.001
Histopathologic review of granulomatous inflammation
Abstract
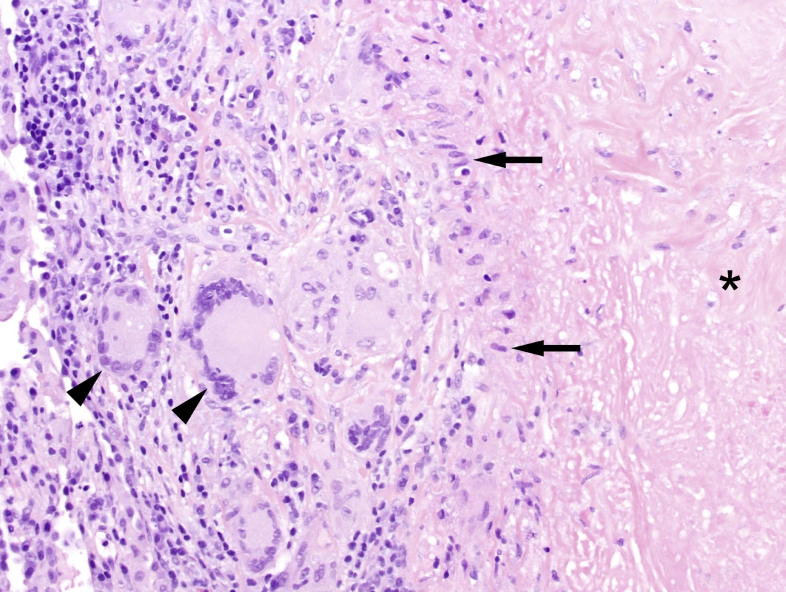
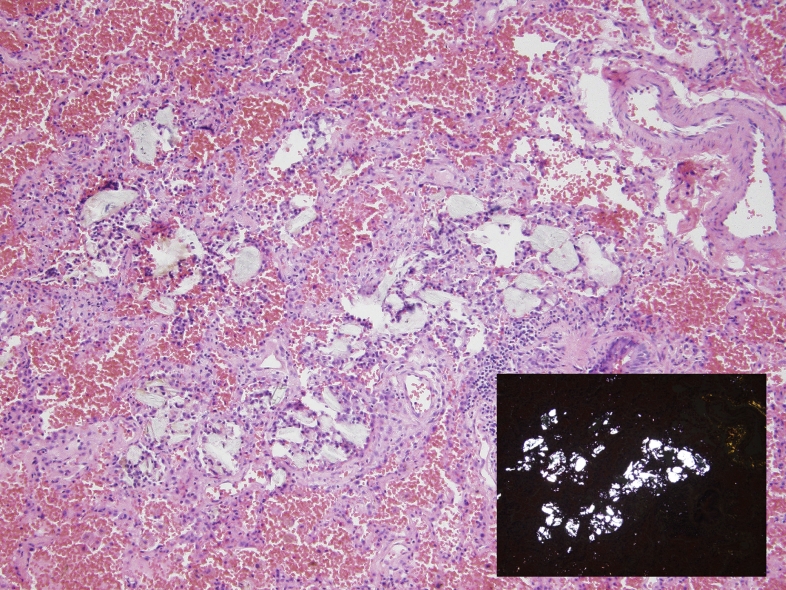
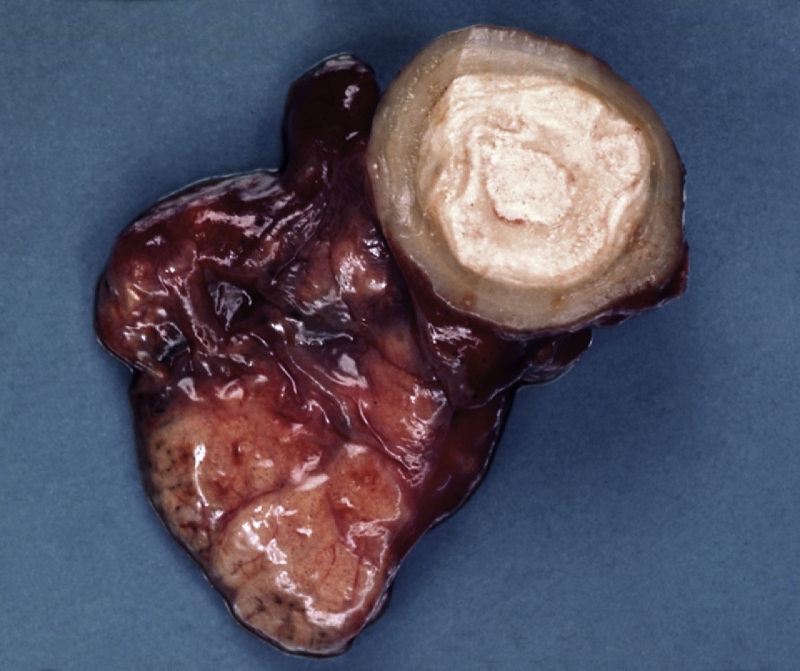
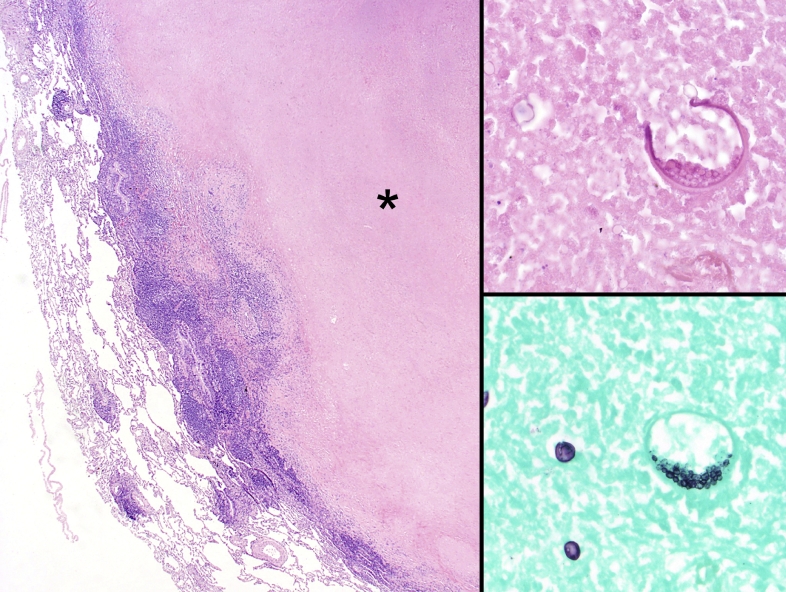
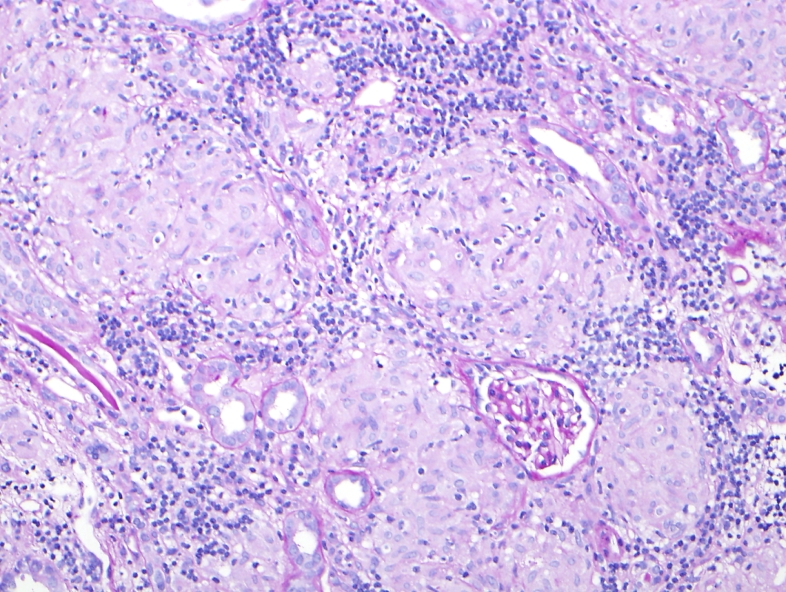
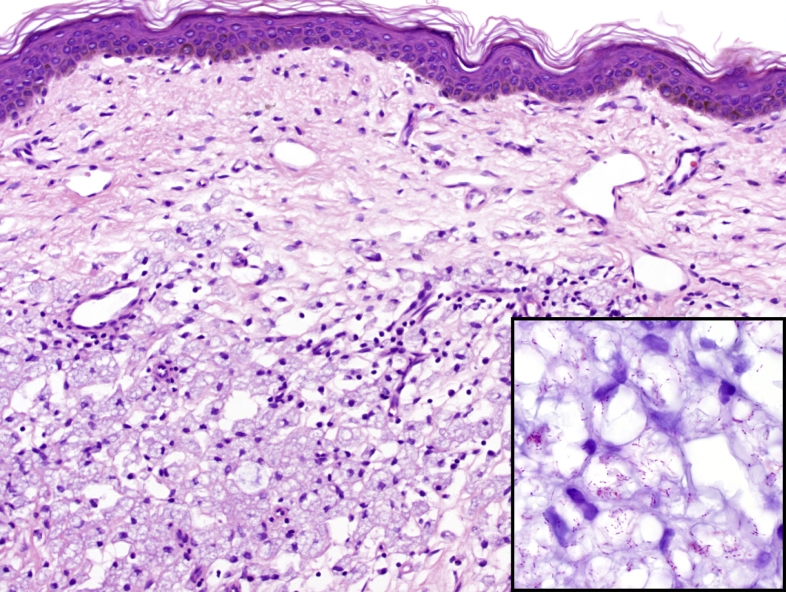
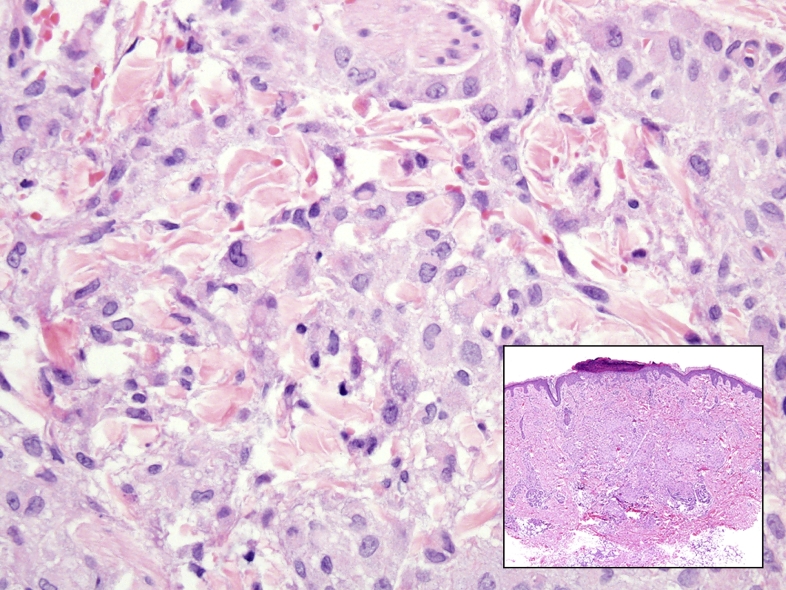
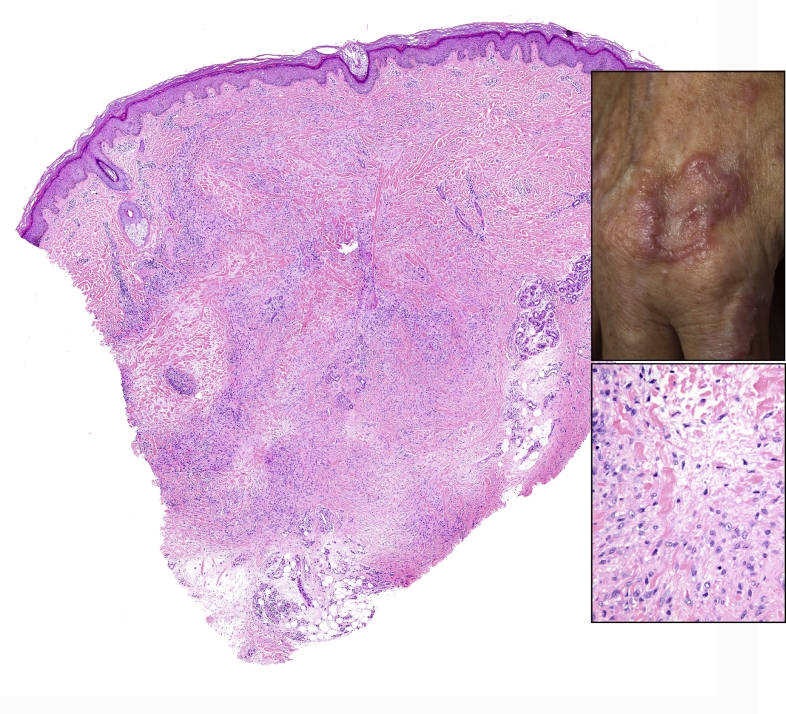
Granulomatous inflammation is a histologic pattern of tissue reaction which appears following cell injury. Granulomatous inflammation is caused by a variety of conditions including infection, autoimmune, toxic, allergic, drug, and neoplastic conditions. The tissue reaction pattern narrows the pathologic and clinical differential diagnosis and subsequent clinical management. Common reaction patterns include necrotizing granulomas, non necrotizing granulomas, suppurative granulomas, diffuse granulomatous inflammation, and foreign body giant cell reaction. Prototypical examples of necrotizing granulomas are seen with mycobacterial infections and non-necrotizing granulomas with sarcoidosis. However, broad differential diagnoses exist within each category. Using a pattern based algorithmic approach, identification of the etiology becomes apparent when taken with clinical context. The pulmonary system is one of the most commonly affected sites to encounter granulomatous inflammation. Infectious causes of granuloma are most prevalent with mycobacteria and dimorphic fungi leading the differential diagnoses. Unlike the lung, skin can be affected by several routes, including direct inoculation, endogenous sources, and hematogenous spread. This broad basis of involvement introduces a variety of infectious agents, which can present as necrotizing or non-necrotizing granulomatous inflammation. Non-infectious etiologies require a thorough clinicopathologic review to narrow the scope of the pathogenesis which include: foreign body reaction, autoimmune, neoplastic, and drug related etiologies. Granulomatous inflammation of the kidney, often referred to as granulomatous interstitial nephritis (GIN) is unlike organ systems such as the skin or lungs. The differential diagnosis of GIN is more frequently due to drugs and sarcoidosis as compared to infections (fungal and mycobacterial). Herein we discuss the pathogenesis and histologic patterns seen in a variety of organ systems and clinical conditions.
Keywords: Foreign-body; Granuloma; Granulomatous inflammation; Mycobacterial; Sarcoidal; Tuberculous.
© 2017 Published by Elsevier Ltd.
Figures
References
-
- Mukhopadhyay S. Pulmonary necrotizing granulomas of unknown cause: clinical and pathologic analysis of 131 patients with completely resected nodules. Chest. 2013;144(3):813–824. - PubMed
-
- Imhof B.A., Aurrand-Lions M. Adhesion mechanisms regulating the migration of monocytes. Nat Rev Immunol. 2004;4(6):432–444. - PubMed
-
- Kunkel S.L. Cellular and molecular aspects of granulomatous inflammation. Am J Respir Cell Mol Biol. 1989;1(6):439–447. - PubMed
-
- Gordon S., Taylor P.R. Monocyte and macrophage heterogeneity. Nat Rev Immunol. 2005;5(12):953–964. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
