

Reduced-Intensity Chemotherapy in Patients With Advanced-Stage Hodgkin Lymphoma: Updated Results of the Open-Label, International, Randomised Phase 3 HD15 Trial by the German Hodgkin Study Group
- PMID: 31723734
- PMCID: PMC6745969
- DOI: 10.1097/HS9.0000000000000005
Reduced-Intensity Chemotherapy in Patients With Advanced-Stage Hodgkin Lymphoma: Updated Results of the Open-Label, International, Randomised Phase 3 HD15 Trial by the German Hodgkin Study Group
Abstract
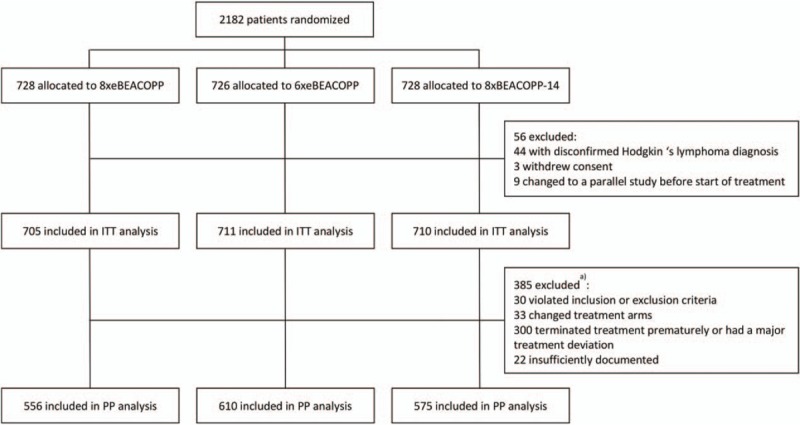
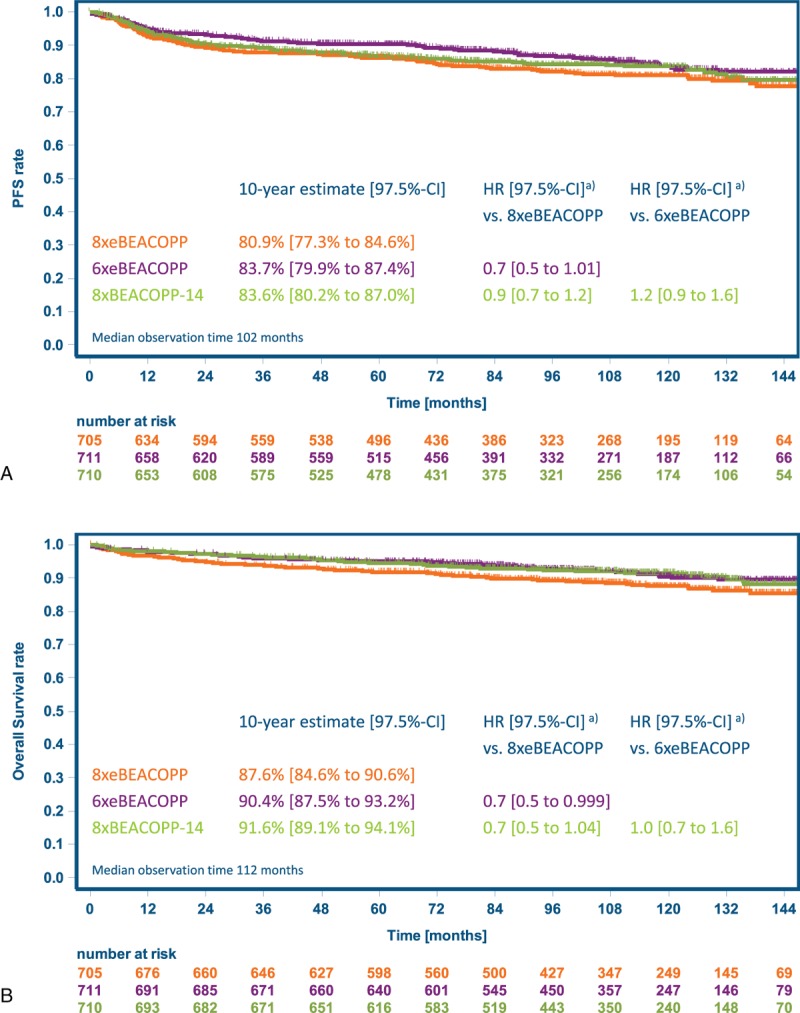
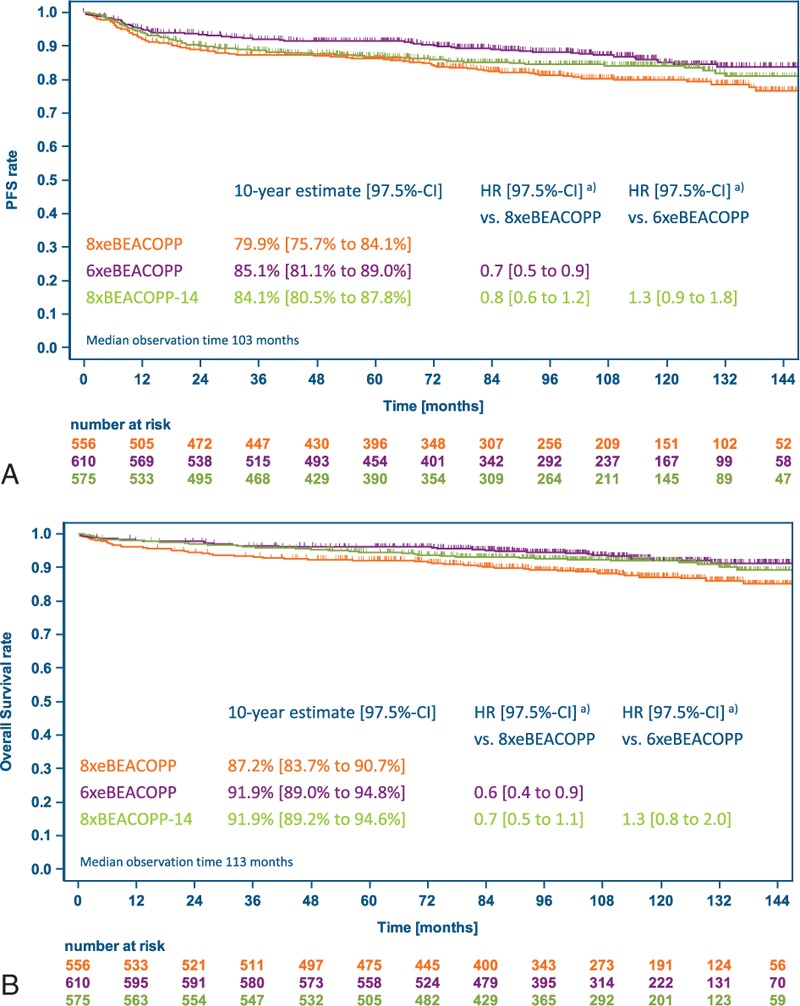
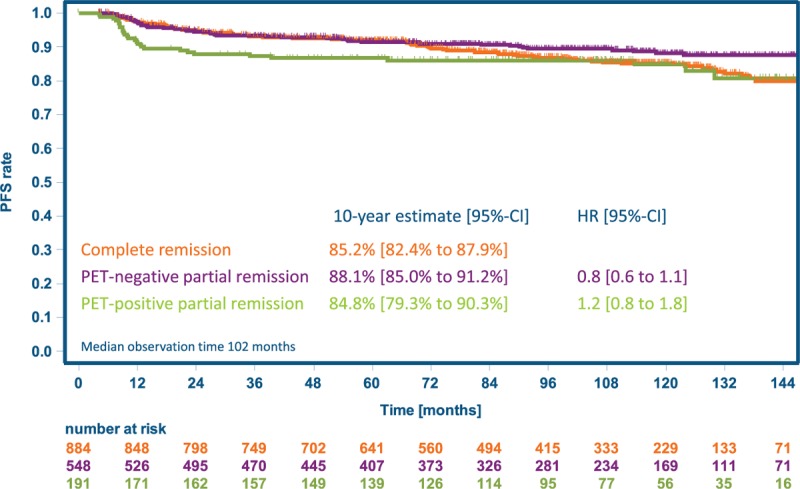
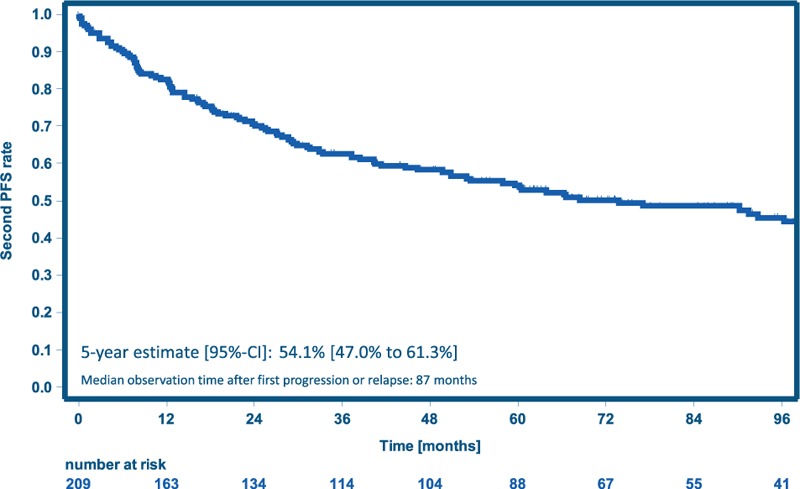
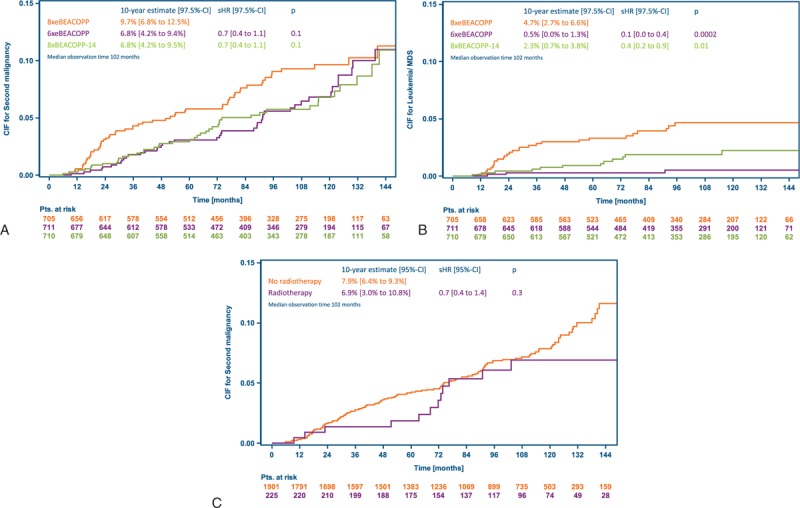
The international, randomized phase 3 HD15 trial established 6xeBEACOPP as standard therapy for patients with newly diagnosed advanced-stage Hodgkin lymphoma (HL) within the German Hodgkin Study Group (GHSG). We performed a follow-up analysis to assess long-term efficacy and safety of this approach. Between 2003 and 2008, 2182 patients aged 18 to 60 years were recruited and randomized in a 1:1:1 ratio between 8 or 6 cycles of eBEACOPP or 8 cycles of the dose-dense BEACOPP-14 regimen, each followed by 30 Gy radiotherapy in case of positron emission tomography (PET)-positive residual lesions ≥2.5 cm. The study aimed at demonstrating non-inferiority regarding efficacy of the 2 experimental arms on a significance level of 2.5% each. The intention-to-treat analysis comprised 2126 patients with a median follow-up of 102 months. Ten-year progression-free survival was 81% (97.5% CI 77-85) with 8xeBEACOPP, 84% (80-87) with 6xeBEACOPP, and 84% (80-87) with 8xBEACOPP-14; the non-inferiority margin of 1.51 for the hazard ratio (HR) could be excluded for both comparisons (6xeBEACOPP, HR = 0.7, 97.5% CI 0.5-1.0; 8xBEACOPP-14, HR = 0.9, 97.5% CI 0.7-1.2). Overall survival at 10 years was 88% (85-91), 90% (88-93), and 92% (89-94), respectively. A total of 142 second malignancies corresponding to 10-year cumulative incidences of 10%, 7%, and 7% and standardized incidence ratios of 4.3, 2.5, and 2.8 were reported for 8xeBEACOPP, 6xeBEACOPP, and 8xBEACOPP-14, respectively. This updated analysis of the HD15 trial thus confirms the efficacy and reports on the long-term safety of a shortened first-line chemotherapy consisting of 6xeBEACOPP followed by PET-guided radiotherapy in advanced-stage HL.
Keywords: Advanced stages; Hodgkin lymphoma; long-term outcome.
Copyright © 2017 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Figures
References
-
- Canellos GP, Anderson JR, Propert KJ, et al. Chemotherapy of advanced Hodgkin's disease with MOPP, ABVD, or MOPP alternating with ABVD. N Engl J Med 1992;327:1478–1484. - PubMed
-
- Gordon LI, Hong F, Fisher RI, et al. Randomized phase III trial of ABVD versus Stanford V with or without radiation therapy in locally extensive and advanced-stage Hodgkin lymphoma: an intergroup study coordinated by the Eastern Cooperative Oncology Group (E2496). J Clin Oncol 2013;31:684–691. - PMC - PubMed
-
- Diehl V, Franklin J, Pfreundschuh M, et al. German Hodgkin's Lymphoma Study Group. Standard and increased-dose BEACOPP chemotherapy compared with COPP-ABVD for advanced Hodgkin's disease. N Engl J Med 2003;348:2386–2395. - PubMed
-
- Borchmann P, Haverkamp H, Diehl V, et al. Eight cycles of escalated-dose BEACOPP compared with four cycles of escalated-dose BEACOPP followed by four cycles of baseline-dose BEACOPP with or without radiotherapy in patients with advanced-stage hodgkin's lymphoma: final analysis of the HD12 trial of the German Hodgkin Study Group. J Clin Oncol 2011;29:4234–4242. - PubMed
-
- Engert A, Haverkamp H, Kobe C, et al. German Hodgkin Study Group; Swiss Group for Clinical Cancer Research; Arbeitsgemeinschaft Medikamentöse Tumortherapie. Reduced-intensity chemotherapy and PET-guided radiotherapy in patients with advanced stage Hodgkin's lymphoma (HD15 trial): a randomised, open-label, phase 3 non-inferiority trial. Lancet 2012;379:1791–1799. - PubMed
LinkOut - more resources
Full Text Sources