Potential for dose reduction in CT emphysema densitometry with post-scan noise reduction: a phantom study
- PMID: 31724436
- PMCID: PMC6948080
- DOI: 10.1259/bjr.20181019
Potential for dose reduction in CT emphysema densitometry with post-scan noise reduction: a phantom study
Abstract
Objective: The aim of this phantom study was to investigate the effect of scan parameters and noise suppression techniques on the minimum radiation dose for acceptable image quality for CT emphysema densitometry.
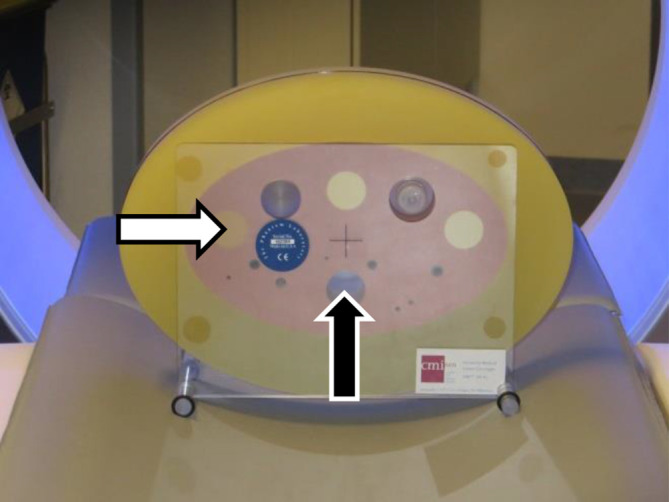
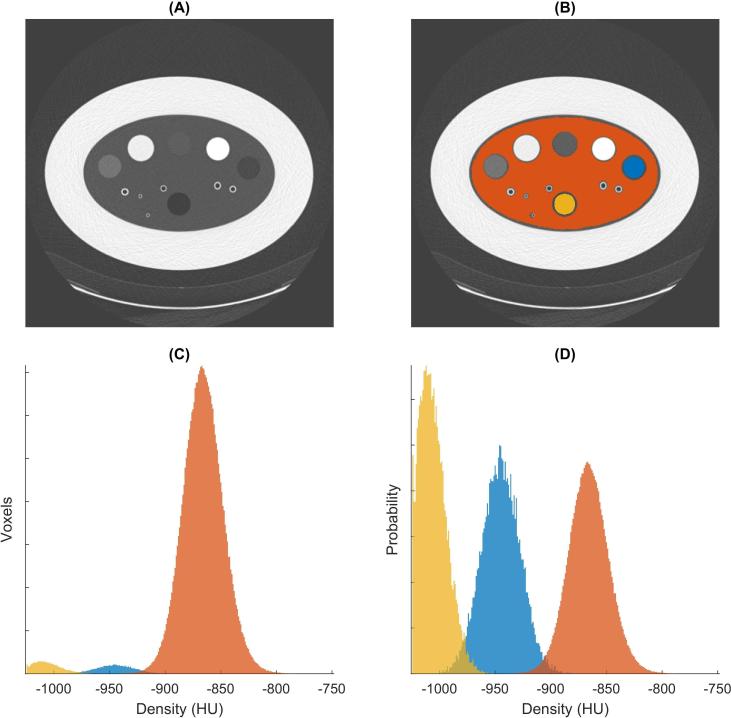
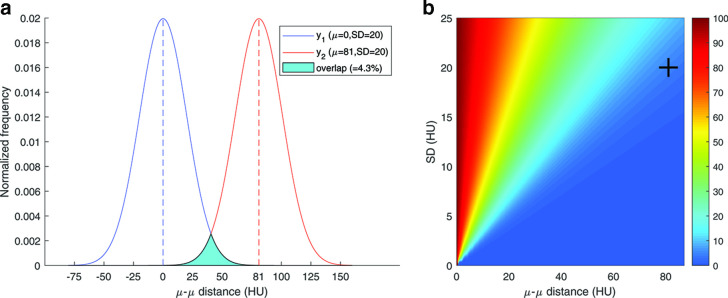
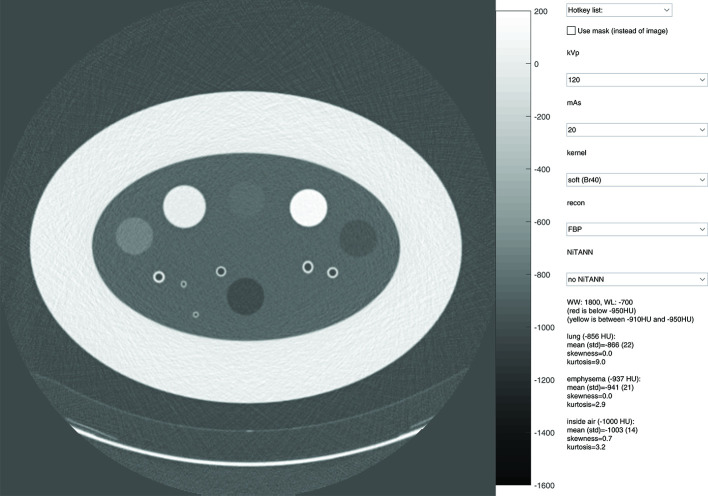
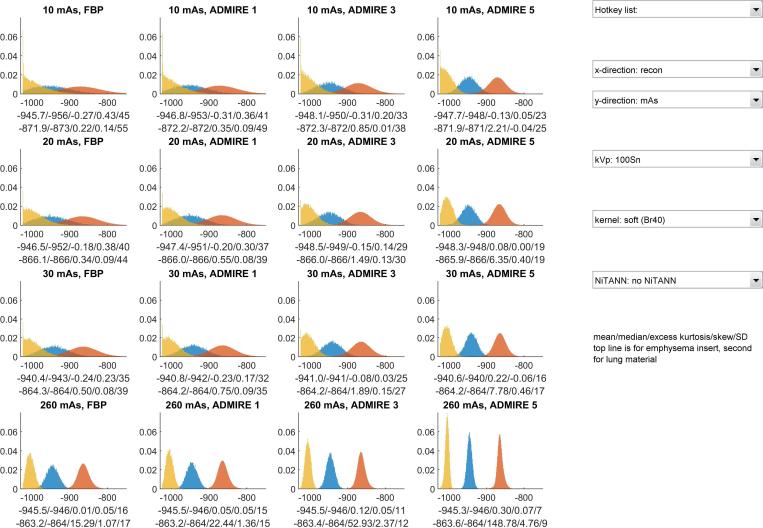
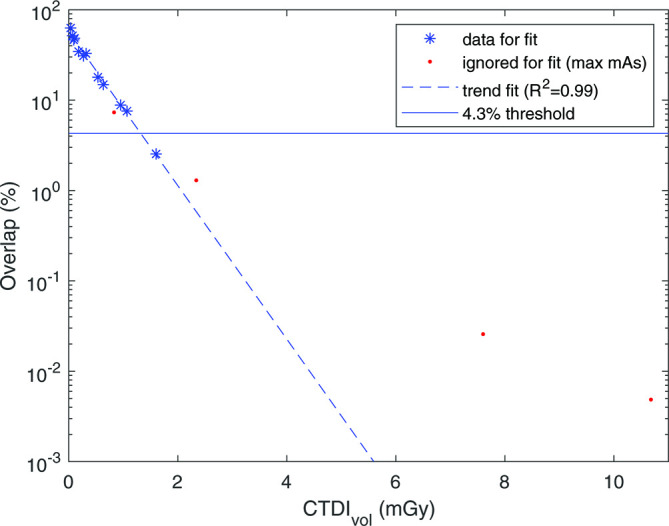
Methods: The COPDGene phantom was scanned on a third generation dual-source CT system with 16 scan setups (CTDIvol 0.035-10.680 mGy). Images were reconstructed at 1.0/0.7 mm slice thickness/increment, with three kernels (one soft, two hard), filtered backprojection and three grades of third-generation iterative reconstruction (IR). Additionally, deep learning-based noise suppression software was applied. Main outcomes: overlap in area of the normalized histograms of CT density for the emphysema insert and lung material, and the radiation dose required for a maximum of 4.3% overlap (defined as acceptable image quality).
Results: In total, 384 scan reconstructions were analyzed. Decreasing radiation dose resulted in an exponential increase of the overlap in normalized histograms of CT density. The overlap was 11-91% for the lowest dose setting (CTDIvol 0.035mGy). The soft kernel reconstruction showed less histogram overlap than hard filter kernels. IR and noise suppression also reduced overlap. Using intermediate grade IR plus noise suppression software allowed for 85% radiation dose reduction while maintaining acceptable image quality.
Conclusion: CT density histogram overlap can quantify the degree of discernibility of emphysema and healthy lung tissue. Noise suppression software, IR, and soft reconstruction kernels substantially decrease the dose required for acceptable image quality.
Advances in knowledge: Noise suppression software, IR, and soft reconstruction kernels allow radiation dose reduction by 85% while still allowing differentiation between emphysema and normal lung tissue.
Figures