

Treatment of an extracranial internal carotid artery aneurysm with a flow-diverting stent
- PMID: 31724620
- PMCID: PMC6849977
- DOI: 10.1016/j.jvsc.2015.04.016
Treatment of an extracranial internal carotid artery aneurysm with a flow-diverting stent
Abstract
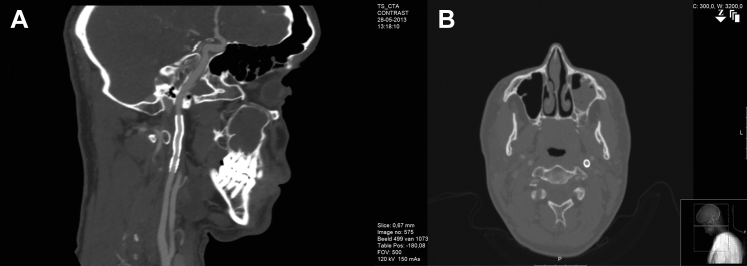
No evidenced-based guidelines exist for the treatment of extracranial carotid artery aneurysms (ECAAs). The "gold standard" for symptomatic ECAAs is surgical intervention. In distally located ECAAs just below the base of the skull, endovascular monotherapy may be beneficial. We present the case of a 21-year-old man with a symptomatic saccular aneurysm in the distal internal carotid artery receiving a flow-diverting stent. The stent was successfully positioned without adverse procedural events. At 6 months, computed tomography angiography revealed secondary occlusion of the aneurysm without further complications. The flow-diverting stent may serve as an additional treatment option for the endovascular specialist considering invasive treatment in patients with an ECAA.
© 2015 The Authors.
Figures


References
-
- Welleweerd J.C., Moll F.L., de Borst G.J. Technical options for the treatment of extracranial carotid aneurysms. Expert Rev Cardiovasc Ther. 2012;10:925–931. - PubMed
-
- Longo G.M., Kibbe M.R. Aneurysms of the carotid artery. Semin Vasc Surg. 2005;18:178–183. - PubMed
-
- Choudhary A.S., Evans R.J., Naik D.K., Tripathi R.K., Wickremesekera J.K. Surgical management of extracranial carotid artery aneurysms. ANZ J Surg. 2009;79:281–287. - PubMed
-
- Attigah N., Kulkens S., Zausig N., Hansmann J., Ringleb P., Hakimi M. Surgical therapy of extracranial carotid artery aneurysms: long-term results over a 24-year period. Eur J Vasc Endovasc Surg. 2009;37:127–133. - PubMed
-
- Malikov S., Thomassin J.M., Magnan P.E., Keshelava G., Bartoli M., Branchereau A. Open surgical reconstruction of the internal carotid artery aneurysm at the base of the skull. J Vasc Surg. 2010;51:323–329. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources