

Non-neoplastic Polyps of the Gallbladder: A Clinicopathologic Analysis of 447 Cases
- PMID: 31725469
- PMCID: PMC8693758
- DOI: 10.1097/PAS.0000000000001405
Non-neoplastic Polyps of the Gallbladder: A Clinicopathologic Analysis of 447 Cases
Abstract
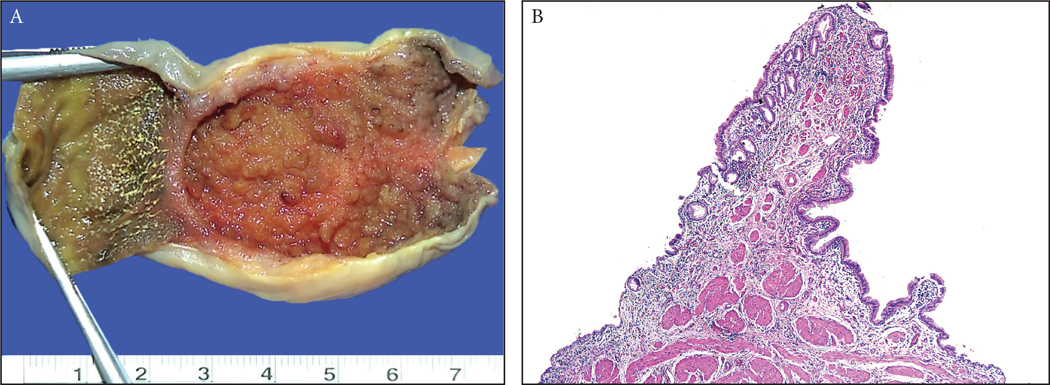
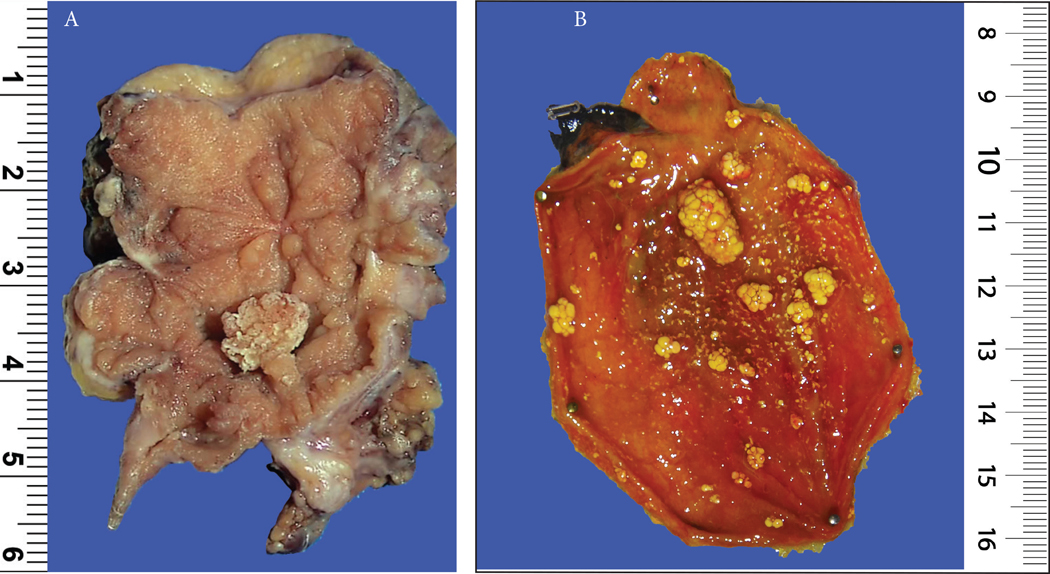
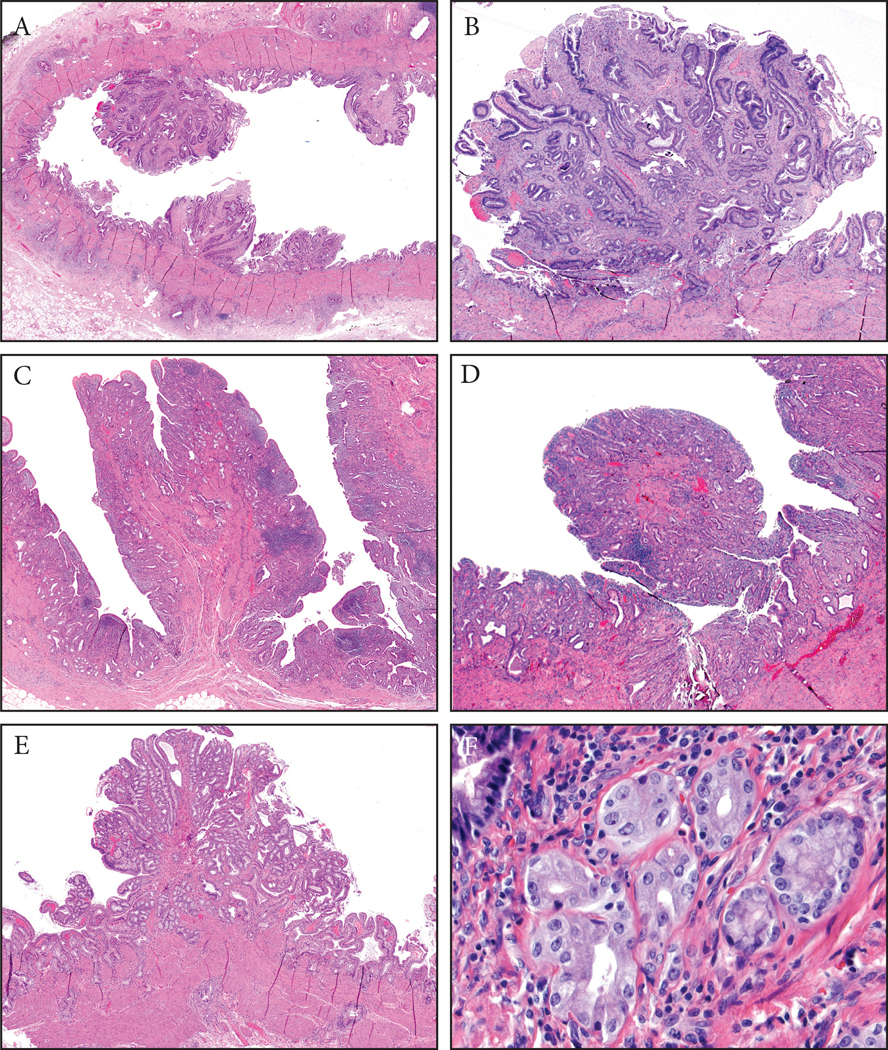
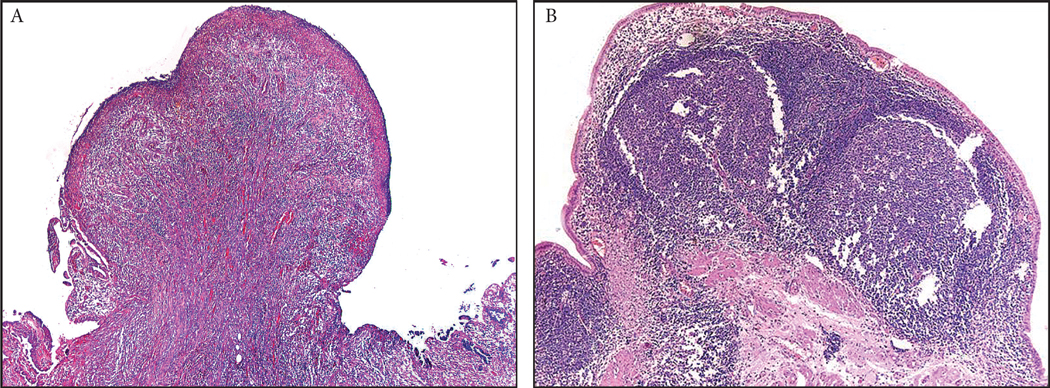
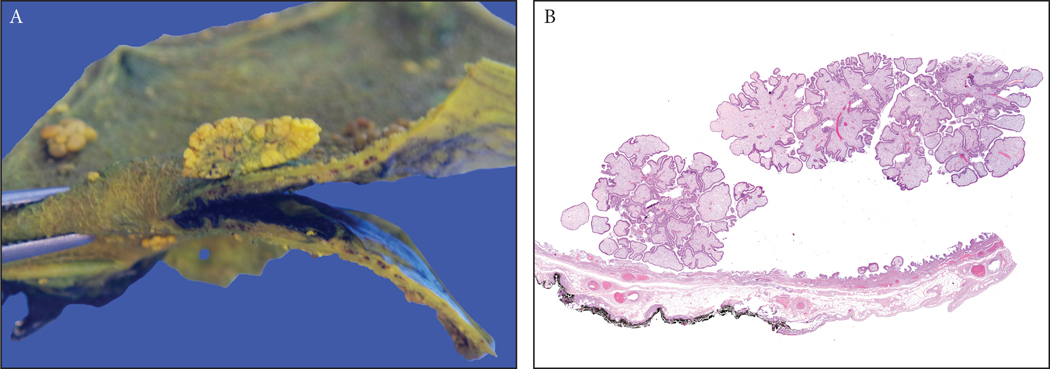
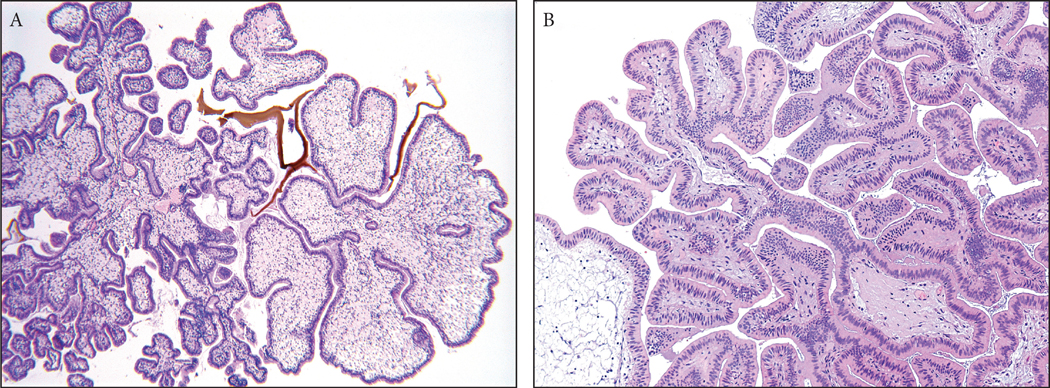
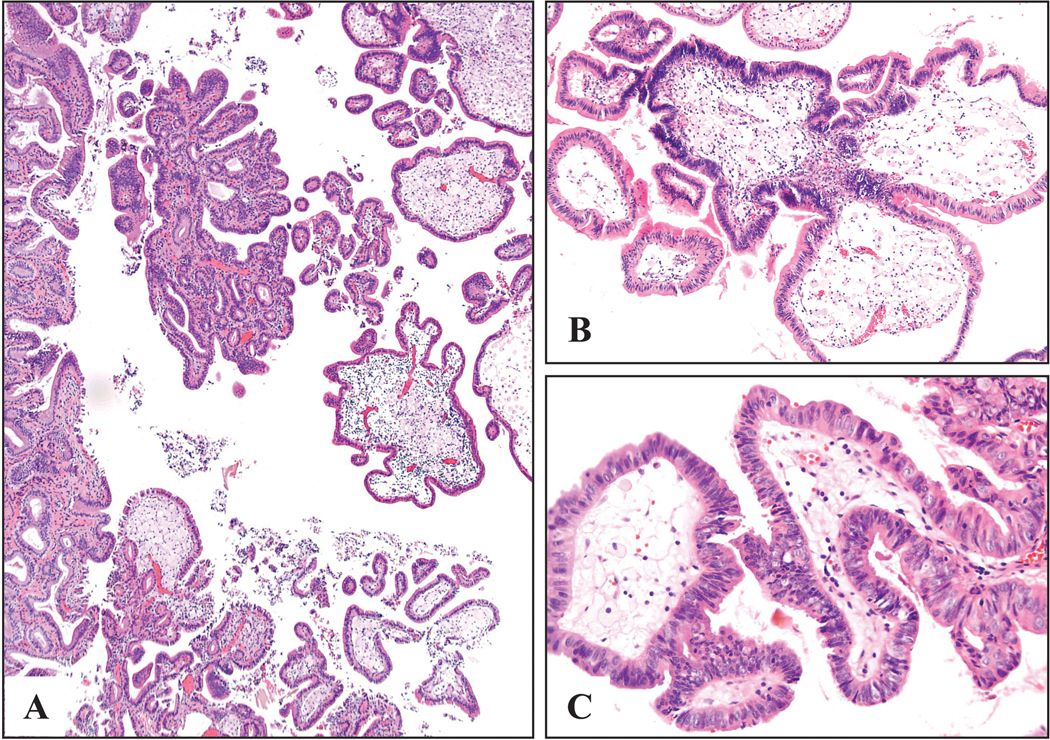
There is no systematic histopathologic analysis of non-neoplastic polyps in the gallbladder. In this study, in addition to a computer search for cases designated as "polyp," a systematic review of 2533 consecutive routinely sampled archival and 203 totally submitted prospective cholecystectomies were analyzed for >2 mm polyps (cut-off was based on radiologic sensitivity). A total of 447 non-neoplastic polyps were identified. The frequency was 3% in archival cases and 5% in totally submitted cases. Only 21 (5%) were ≥1 cm. The average age was 52 years, and the female to male ratio was 3.1. Two distinct categories were delineated: (1) injury-related polyps (n=273): (a) Fibro(myo)glandular polyps (n=214) were small (mean=0.4 cm), broad-based, often multiple (45%), almost always (98%) gallstone-associated, and were composed of a mixture of (myo)fibroblastic tissue/lobular glandular units with chronic cholecystitis. Dysplasia seen in 9% seemed to be secondary involvement. (b) Metaplastic pyloric glands forming polypoid collections (n=42). (c) Inflammatory-type polyps associated with acute/subacute injury (11 granulation tissue, 3 xanthogranulomatous, 3 lymphoid). (2) Cholesterol polyps (n=174) occurred in uninjured gallbladders, revealing a very thin stalk, edematous cores devoid of glands but with cholesterol-laden macrophages in 85%, and cholesterolosis in the uninvolved mucosa in 60%. Focal low-grade dysplasia was seen in 3%, always confined to the polyp, unaccompanied by carcinoma. In conclusion, non-neoplastic polyps are seen in 3% of cholecystectomies and are often small. Injury-related fibromyoglandular polyps are the most common. Cholesterol polyps have distinctive cauliflower architecture, often in a background of uninjured gallbladders with cholesterolosis and may lack the cholesterol-laden macrophages in the polyp itself. Although dysplastic changes can involve non-neoplastic polyps, they do not seem to be the cause of invasive carcinoma by themselves.
Conflict of interest statement
- Conflict of Interest: Authors declare that they have no conflict of interest to disclose.
Figures
References
-
- Wiles R, Thoeni RF, Barbu ST, et al. Management and follow-up of gallbladder polyps : Joint guidelines between the European Society of Gastrointestinal and Abdominal Radiology (ESGAR), European Association for Endoscopic Surgery and other Interventional Techniques (EAES), International Society of Digestive Surgery - European Federation (EFISDS) and European Society of Gastrointestinal Endoscopy (ESGE). Eur. Radiol. 2017;27:3856–3866. doi:10.1007/s00330-017-4742-y. - DOI - PMC - PubMed
-
- Albores-Saavedra J, Henson DE. Tumors of the Gallbladder and Extrahepatic Bile Ducts. In: Atlas of Tumor Pathology. 2nd series. Washington, DC: Armed Forces Institute of Pathology; 1986.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
