

Risk-Adapted Starting Age of Screening for Relatives of Patients With Breast Cancer
- PMID: 31725845
- PMCID: PMC6865319
- DOI: 10.1001/jamaoncol.2019.3876
Risk-Adapted Starting Age of Screening for Relatives of Patients With Breast Cancer
Erratum in
-
Error in Author's Name.JAMA Oncol. 2020 Jan 1;6(1):162. doi: 10.1001/jamaoncol.2019.5986. JAMA Oncol. 2020. PMID: 31830231 Free PMC article. No abstract available.
Abstract
Importance: Breast cancer screening guidelines acknowledge the need for earlier screening for women at increased risk but provide limited guidance for women with a family history of breast cancer. A risk-adapted starting age of screening for relatives of patients with breast cancer may help supplement current screening guidelines.
Objective: To identify the risk-adapted starting age of breast cancer screening on the basis of a woman's detailed family history.
Design, setting, and participants: This nationwide cohort study analyzed data recorded in the Swedish family-cancer data sets. All women born from 1932 onward and with at least 1 known first-degree relative (FDR) were included (N = 5 099 172). Data from January 1, 1958, to December 31, 2015, were collected. Data were analyzed from October 1, 2017, to March 31, 2019.
Exposures: Family history of breast cancer in FDRs and second-degree relatives (SDRs).
Main outcomes and measures: Primary invasive breast cancer diagnosis and the age at which women with different constellations of family history attained the risk level at which breast screening is usually recommended.
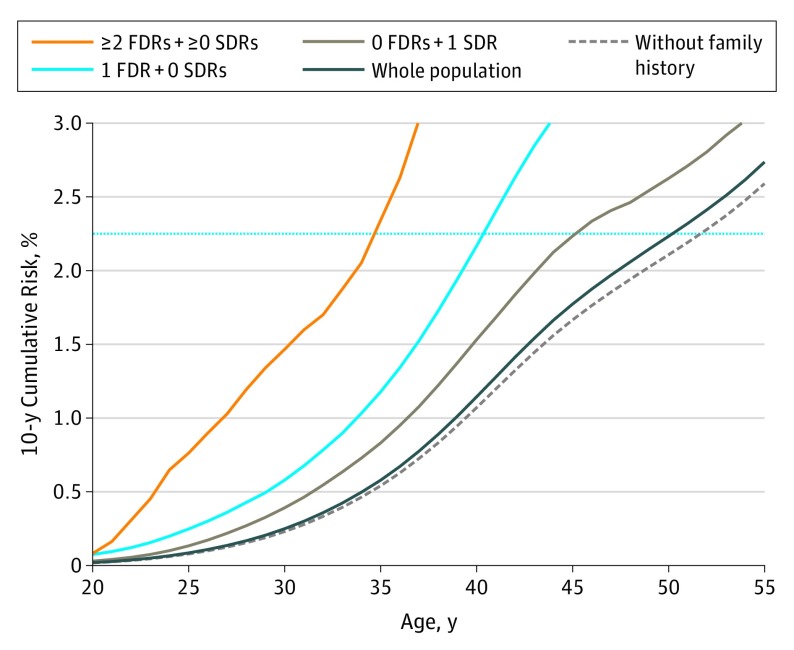
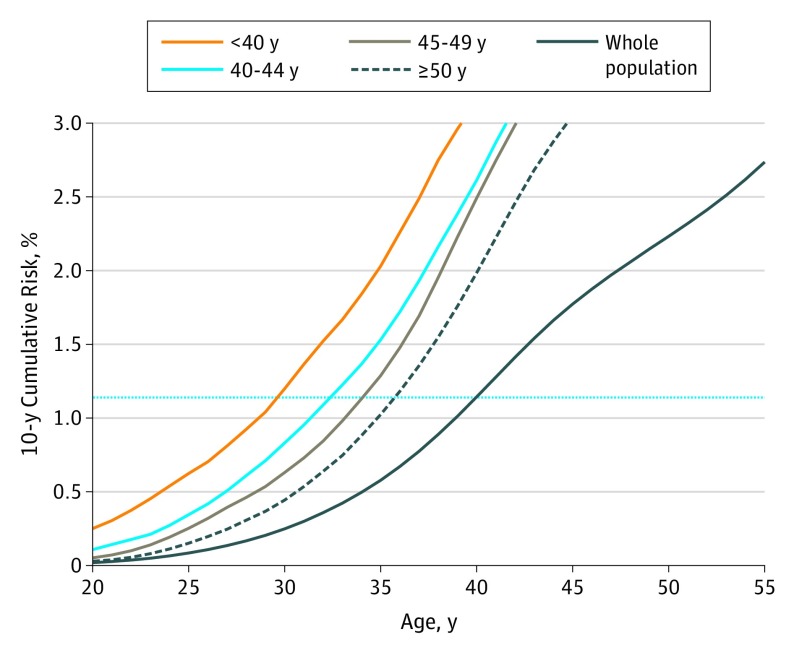
Results: Of the 5 099 172 women included in the study, 118 953 (2.3%) received a diagnosis of primary invasive breast cancer. A total of 102 751 women (86.4%; mean [SD] age at diagnosis, 55.9 [11.1] years) did not have family history of breast cancer in FDRs and SDRs at the time of their diagnosis. Risk-adapted starting age of breast cancer screening varied by number of FDRs and SDRs with breast cancer diagnosis and the age at diagnosis of the FDRs. For example, for screening recommendation at age 50 years for the general population (2.2% 10-year cumulative risk), women with multiple affected FDRs, with the youngest affected relative receiving a diagnosis before age 50 years, reached the benchmark risk level at age 27 years. When the youngest relative received a diagnosis after age 50 years, however, this risk level was attained at age 36 years.
Conclusions and relevance: This study identifies possible risk-based starting ages for breast cancer screening based on population-based registers. These results may serve as high-quality evidence to supplement current screening guidelines for relatives of patients with breast cancer.
Conflict of interest statement
Figures
Comment in
-
Toward Risk-Stratified Breast Cancer Screening: Considerations for Changes in Screening Guidelines.JAMA Oncol. 2020 Jan 1;6(1):31-33. doi: 10.1001/jamaoncol.2019.3820. JAMA Oncol. 2020. PMID: 31725821 Free PMC article. No abstract available.
-
Breast cancer screening programs: does one risk fit all?Quant Imaging Med Surg. 2020 Apr;10(4):886-890. doi: 10.21037/qims.2020.03.14. Quant Imaging Med Surg. 2020. PMID: 32355656 Free PMC article. No abstract available.
-
Determining the Appropriate Risk-Adapted Screening Age for Familial Breast Cancer.JAMA Oncol. 2020 Jun 1;6(6):933-934. doi: 10.1001/jamaoncol.2020.0286. JAMA Oncol. 2020. PMID: 32379276 No abstract available.
-
Determining the Appropriate Risk-Adapted Screening Age for Familial Breast Cancer-Reply.JAMA Oncol. 2020 Jun 1;6(6):934-935. doi: 10.1001/jamaoncol.2020.0292. JAMA Oncol. 2020. PMID: 32379279 No abstract available.
-
Breast cancer screening: in the era of personalized medicine, age is just a number.Quant Imaging Med Surg. 2020 Dec;10(12):2401-2407. doi: 10.21037/qims-2020-26. Quant Imaging Med Surg. 2020. PMID: 33269240 Free PMC article. No abstract available.
References
-
- Ferlay JSI, Ervik M, Dikshit R, et al. . Cancer Incidence and Mortality Worldwide. Lyon, France: International Agency for Research on Cancer; 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
