

Novel risk genes and mechanisms implicated by exome sequencing of 2572 individuals with pulmonary arterial hypertension
- PMID: 31727138
- PMCID: PMC6857288
- DOI: 10.1186/s13073-019-0685-z
Novel risk genes and mechanisms implicated by exome sequencing of 2572 individuals with pulmonary arterial hypertension
Erratum in
-
Correction to: Novel risk genes and mechanisms implicated by exome sequencing of 2572 individuals with pulmonary arterial hypertension.Genome Med. 2022 Feb 7;14(1):12. doi: 10.1186/s13073-022-01014-0. Genome Med. 2022. PMID: 35130931 Free PMC article. No abstract available.
Abstract
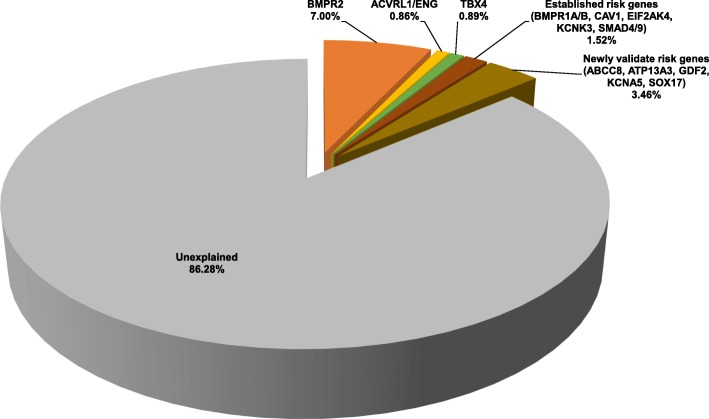
Background: Group 1 pulmonary arterial hypertension (PAH) is a rare disease with high mortality despite recent therapeutic advances. Pathogenic remodeling of pulmonary arterioles leads to increased pulmonary pressures, right ventricular hypertrophy, and heart failure. Mutations in bone morphogenetic protein receptor type 2 and other risk genes predispose to disease, but the vast majority of non-familial cases remain genetically undefined.
Methods: To identify new risk genes, we performed exome sequencing in a large cohort from the National Biological Sample and Data Repository for PAH (PAH Biobank, n = 2572). We then carried out rare deleterious variant identification followed by case-control gene-based association analyses. To control for population structure, only unrelated European cases (n = 1832) and controls (n = 12,771) were used in association tests. Empirical p values were determined by permutation analyses, and the threshold for significance defined by Bonferroni's correction for multiple testing.
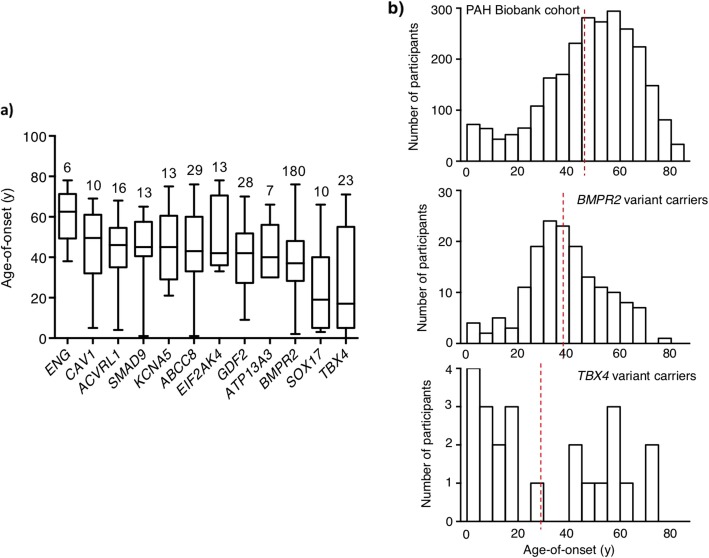
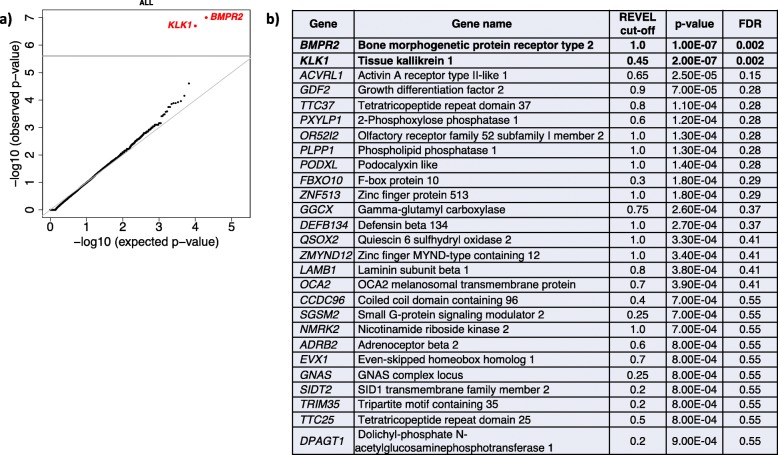
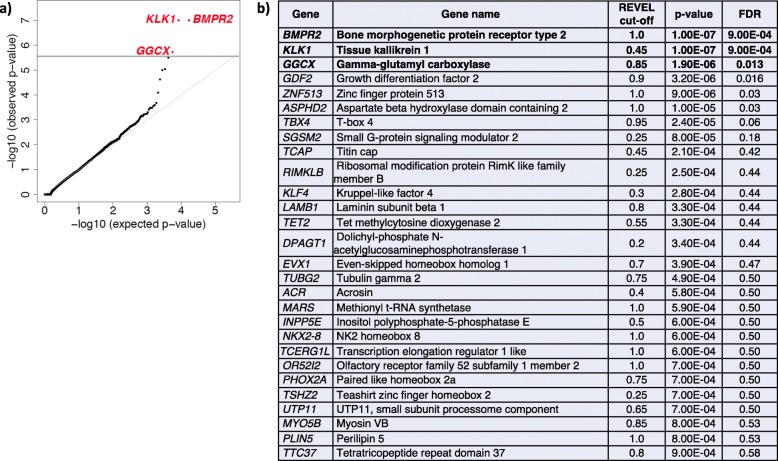
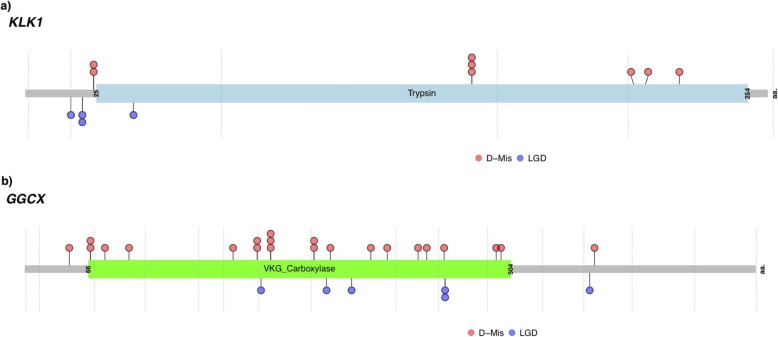
Results: Tissue kallikrein 1 (KLK1) and gamma glutamyl carboxylase (GGCX) were identified as new candidate risk genes for idiopathic PAH (IPAH) with genome-wide significance. We note that variant carriers had later mean age of onset and relatively moderate disease phenotypes compared to bone morphogenetic receptor type 2 variant carriers. We also confirmed the genome-wide association of recently reported growth differentiation factor (GDF2) with IPAH and further implicate T-box 4 (TBX4) with child-onset PAH.
Conclusions: We report robust association of novel genes KLK1 and GGCX with IPAH, accounting for ~ 0.4% and 0.9% of PAH Biobank cases, respectively. Both genes play important roles in vascular hemodynamics and inflammation but have not been implicated in PAH previously. These data suggest new genes, pathogenic mechanisms, and therapeutic targets for this lethal vasculopathy.
Keywords: Case-control association testing; Exome sequencing; Genetics; Pulmonary arterial hypertension.
Conflict of interest statement
CG-J is a full-time employee of the Regeneron Genetics Center from Regeneron Pharmaceuticals Inc. and receives stock options as part of compensation. The remaining authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
