

Classification of osteonecrosis of the femoral head: Who should have surgery?
- PMID: 31728183
- PMCID: PMC6825048
- DOI: 10.1302/2046-3758.810.BJR-2019-0022.R1
Classification of osteonecrosis of the femoral head: Who should have surgery?
Abstract
Objectives: Using a simple classification method, we aimed to estimate the collapse rate due to osteonecrosis of the femoral head (ONFH) in order to develop treatment guidelines for joint-preserving surgeries.
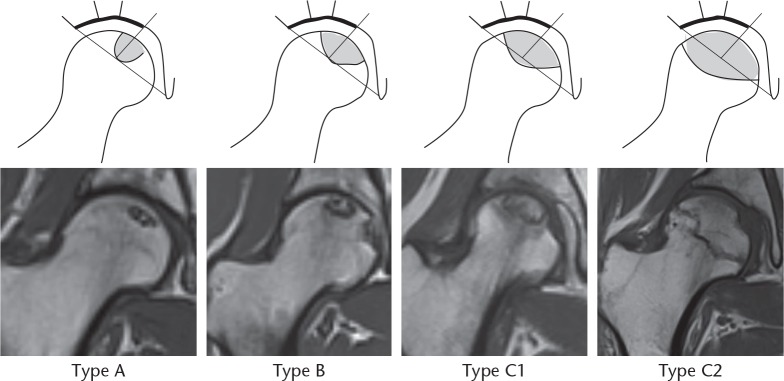
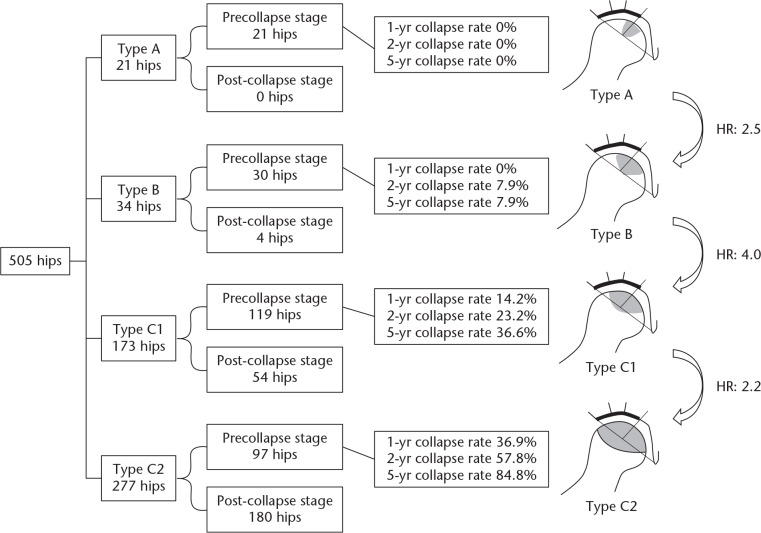
Methods: We retrospectively analyzed 505 hips from 310 patients (141 men, 169 women; mean age 45.5 years (sd 14.9; 15 to 86)) diagnosed with ONFH and classified them using the Japanese Investigation Committee (JIC) classification. The JIC system includes four visualized types based on the location and size of osteonecrotic lesions on weightbearing surfaces (types A, B, C1, and C2) and the stage of ONFH. The collapse rate due to ONFH was calculated using Kaplan-Meier survival analysis, with radiological collapse/arthroplasty as endpoints.
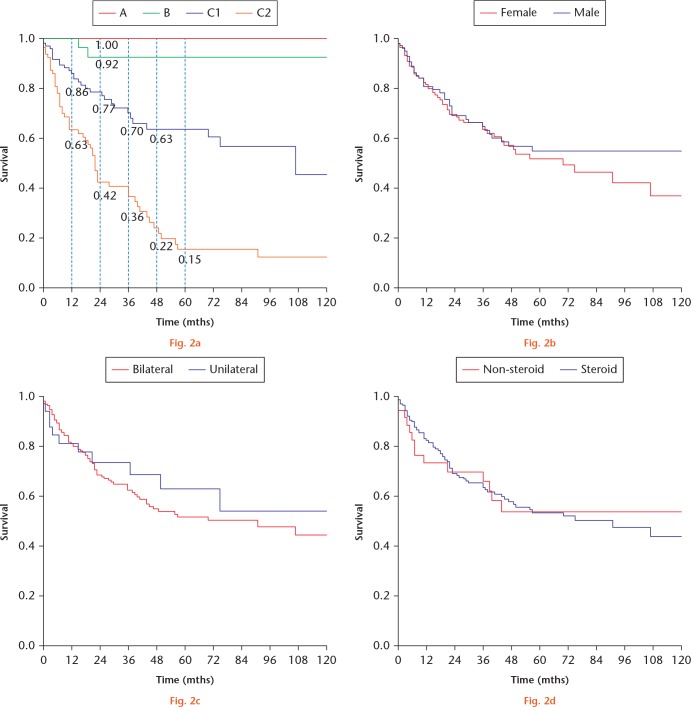
Results: Bilateral cases accounted for 390 hips, while unilateral cases accounted for 115. According to the JIC types, 21 hips were type A, 34 were type B, 173 were type C1, and 277 were type C2. At initial diagnosis, 238/505 hips (47.0%) had already collapsed. Further, the cumulative survival rate was analyzed in 212 precollapsed hips, and the two-year and five-year collapse rates were found to be 0% and 0%, 7.9% and 7.9%, 23.2% and 36.6%, and 57.8% and 84.8% for types A, B, C1, and C2, respectively.
Conclusion: Type A ONFH needs no further treatment, but precollapse type C2 ONFH warrants immediate treatment with joint-preserving surgery. Considering the high collapse rate, our study results justify the importance of early diagnosis and intervention in asymptomatic patients with type C2 ONFH.Cite this article: Y. Kuroda, T. Tanaka, T. Miyagawa, T. Kawai, K. Goto, S. Tanaka, S. Matsuda, H. Akiyama. Classification of osteonecrosis of the femoral head: Who should have surgery?. Bone Joint Res 2019;8:451-458. DOI: 10.1302/2046-3758.810.BJR-2019-0022.R1.
Keywords: Collapse; Femoral head; Joint-preserving surgery; Kaplan–Meier survival analysis; Osteonecrosis.
© 2019 Author(s) et al.
Figures
References
-
- Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR. Nontraumatic osteonecrosis of the femoral head: where do we stand today? A ten-year update. J Bone Joint Surg [Am] 2015;97-A:1604-1627. - PubMed
-
- Mont MA, Zywiel MG, Marker DR, McGrath MS, Delanois RE. The natural history of untreated asymptomatic osteonecrosis of the femoral head: a systematic literature review. J Bone Joint Surg [Am] 2010;92-A:2165-2170. - PubMed
-
- Hernigou P, Poignard A, Nogier A, Manicom O. Fate of very small asymptomatic stage-I osteonecrotic lesions of the hip. J Bone Joint Surg [Am] 2004;86-A:2589-2593. - PubMed
-
- Larson E, Jones LC, Goodman SB, Koo KH, Cui Q. Early-stage osteonecrosis of the femoral head: where are we and where are we going in year 2018? Int Orthop 2018;42:1723-1728. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
