

The BACH classification of long bone osteomyelitis
- PMID: 31728184
- PMCID: PMC6825044
- DOI: 10.1302/2046-3758.810.BJR-2019-0050.R1
The BACH classification of long bone osteomyelitis
Abstract
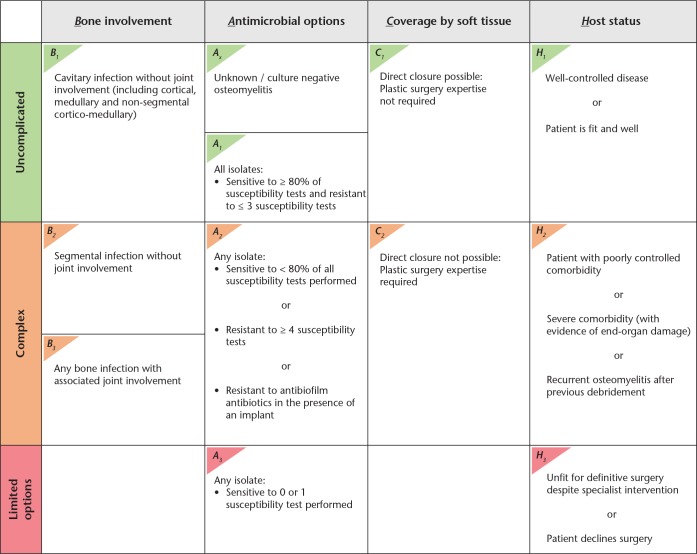
Objectives: The aim of this study was to assess the clinical application of, and optimize the variables used in, the BACH classification of long-bone osteomyelitis.
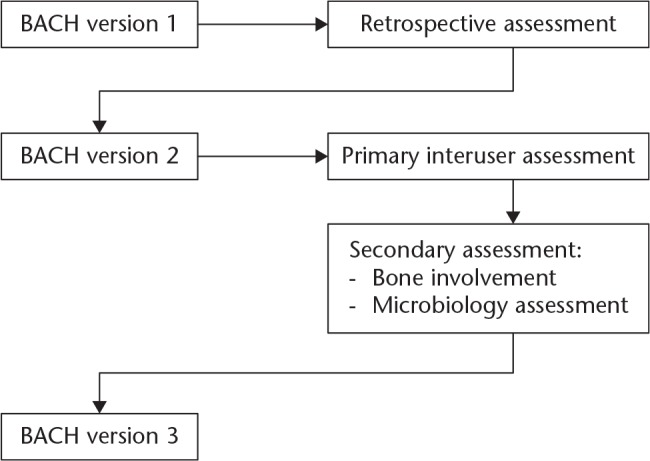
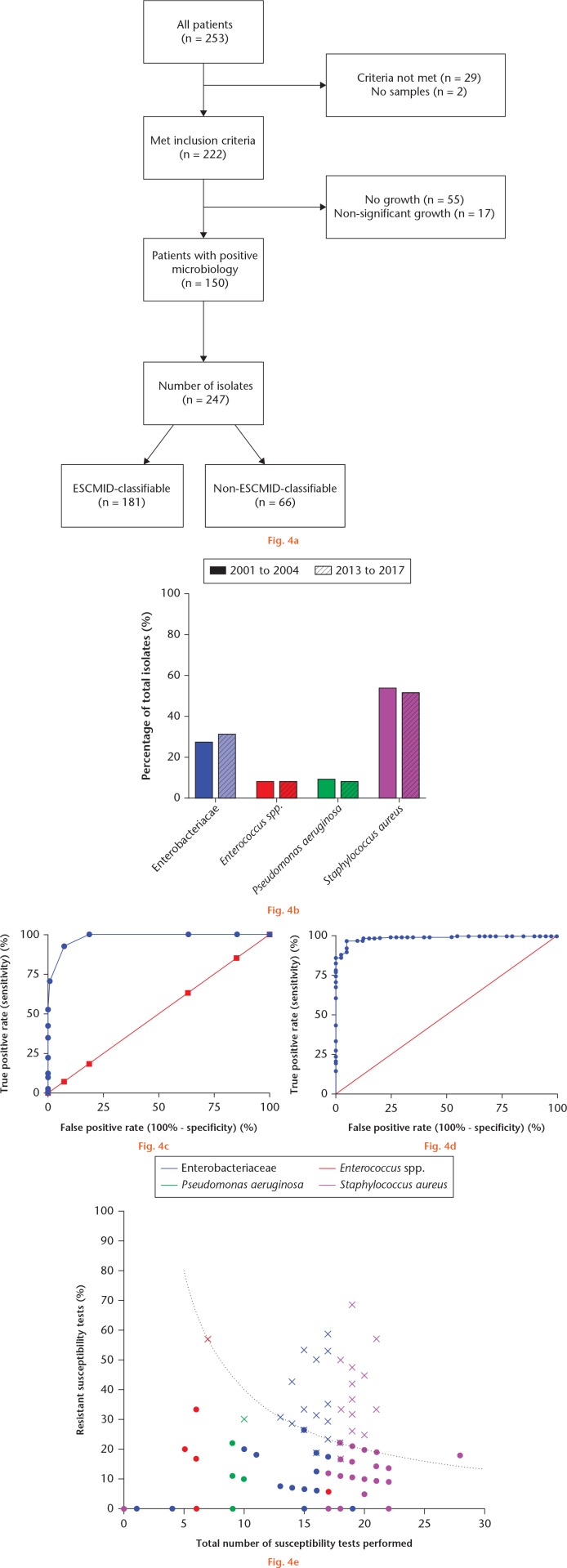
Methods: A total of 30 clinicians from a variety of specialities classified 20 anonymized cases of long-bone osteomyelitis using BACH. Cases were derived from patients who presented to specialist centres in the United Kingdom between October 2016 and April 2017. Accuracy and Fleiss' kappa (Fκ) were calculated for each variable. Bone involvement (B-variable) was assessed further by nine clinicians who classified ten additional cases of long bone osteomyelitis using a 3D clinical imaging package. Thresholds for defining multidrug-resistant (MDR) isolates were optimized using results from a further analysis of 253 long bone osteomyelitis cases.
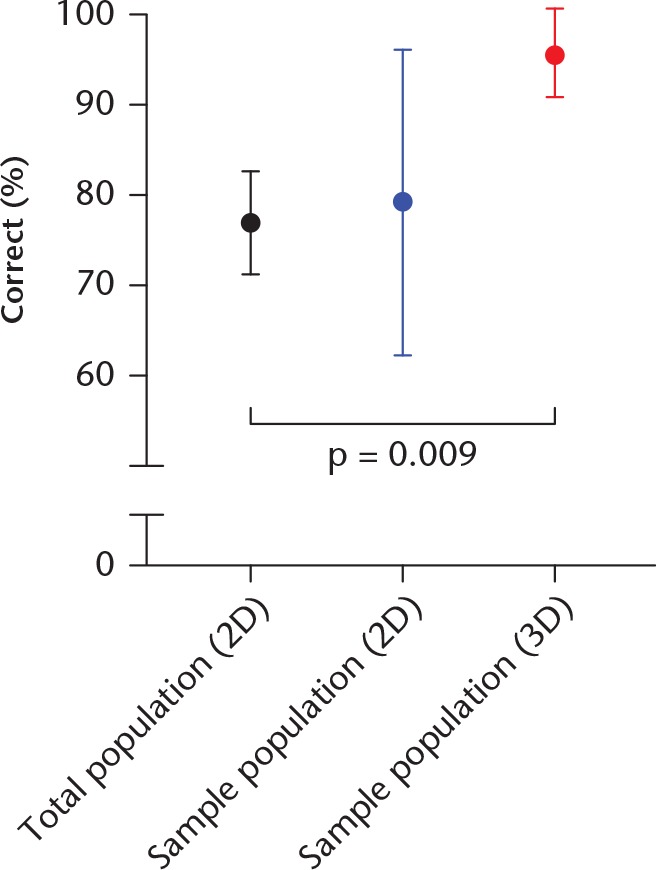
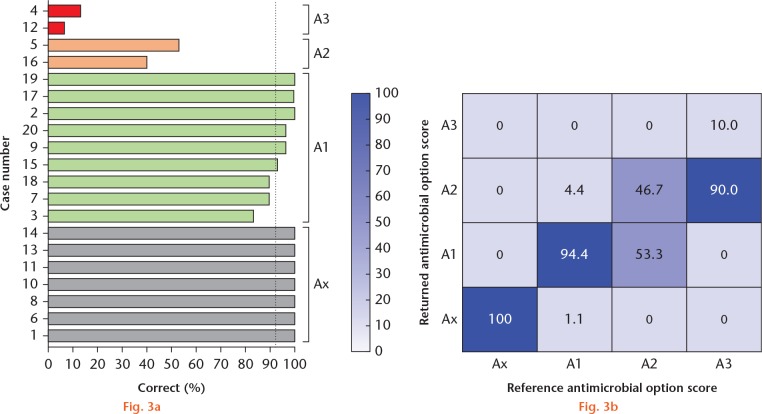
Results: The B-variable had a classification accuracy of 77.0%, which improved to 95.7% when using a 3D clinical imaging package (p < 0.01). The A-variable demonstrated difficulty in the accuracy of classification for increasingly resistant isolates (A1 (non-resistant), 94.4%; A2 (MDR), 46.7%; A3 (extensively or pan-drug-resistant), 10.0%). Further analysis demonstrated that isolates with four or more resistant test results or less than 80% sensitive susceptibility test results had a 98.1% (95% confidence interval (CI) 96.6 to 99.6) and 98.8% (95% CI 98.1 to 100.0) correlation with MDR status, respectively. The coverage of the soft tissues (C-variable) and the host status (H-variable) both had a substantial agreement between users and a classification accuracy of 92.5% and 91.2%, respectively.
Conclusions: The BACH classification system can be applied accurately by users with a variety of clinical backgrounds. Accuracy of B-classification was improved using 3D imaging. The use of the A-variable has been optimized based on susceptibility testing results.Cite this article: A. J. Hotchen, M. Dudareva, J. Y. Ferguson, P. Sendi, M. A. McNally. The BACH classification of long bone osteomyelitis. Bone Joint Res 2019;8:459-468. DOI: 10.1302/2046-3758.810.BJR-2019-0050.R1.
Keywords: Bone and joint infection; Classification; Osteomyelitis.
© 2019 Author(s) et al.
Figures
References
-
- Bose D, Kugan R, Stubbs D, McNally M. Management of infected nonunion of the long bones by a multidisciplinary team. Bone Joint J 2015;97-B:814-817. - PubMed
-
- Magiorakos A-P, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012;18:268-281. - PubMed
-
- Hotchen AJ, Sendi P, McNally M. BACH: a new classification system for long-bone osteomyelitis. Orthopaedic Proceedings 2017;99-B:10.
