

A therapeutic antibody targeting osteoprotegerin attenuates severe experimental pulmonary arterial hypertension
- PMID: 31729368
- PMCID: PMC6858314
- DOI: 10.1038/s41467-019-13139-9
A therapeutic antibody targeting osteoprotegerin attenuates severe experimental pulmonary arterial hypertension
Abstract
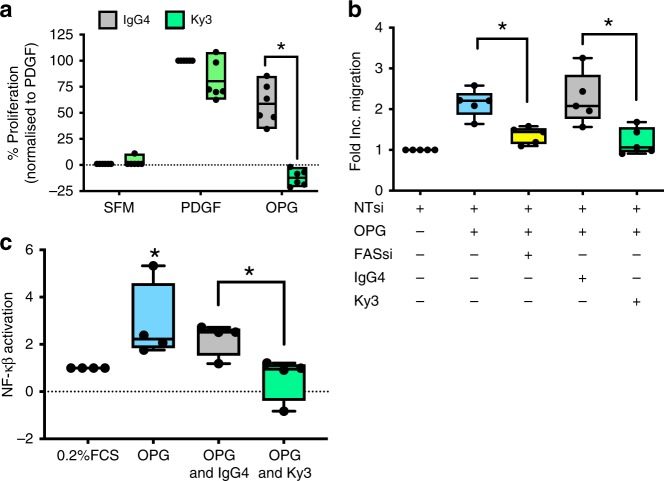
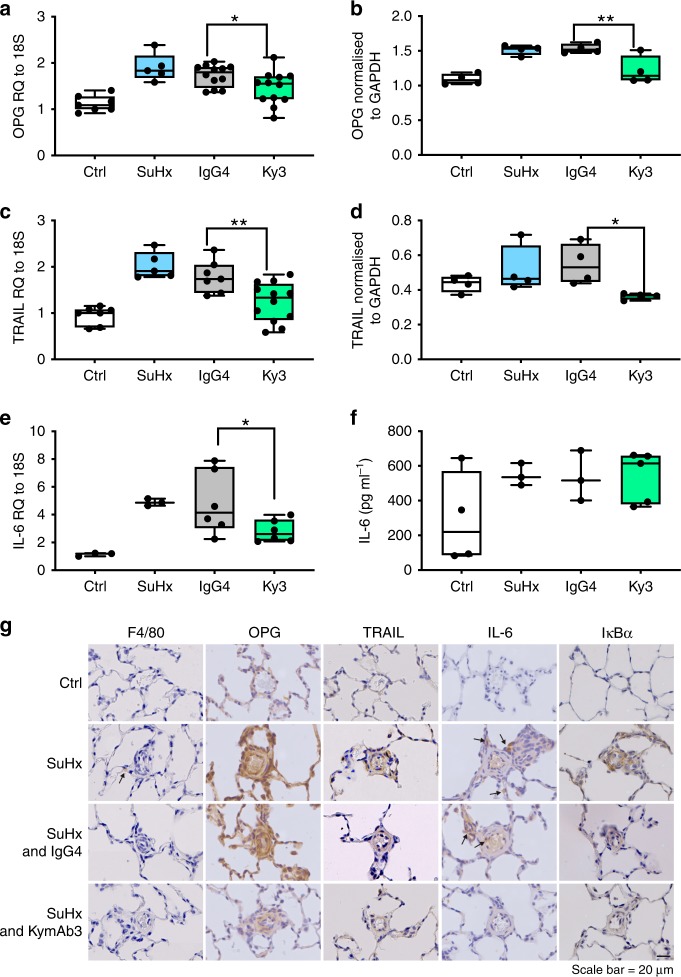
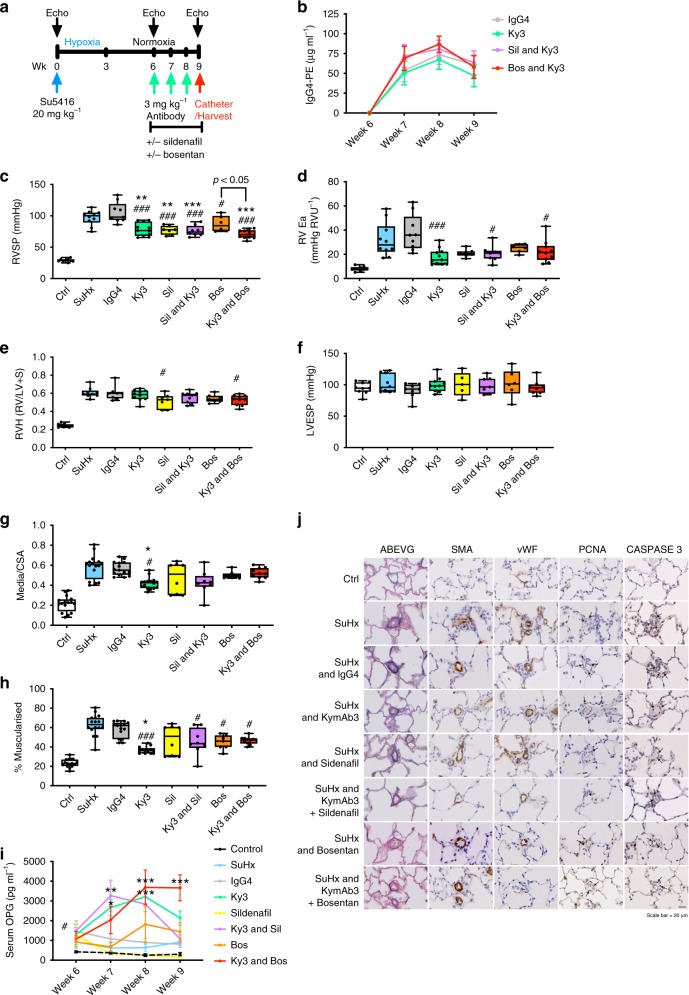
Pulmonary arterial hypertension (PAH) is a rare but fatal disease. Current treatments increase life expectancy but have limited impact on the progressive pulmonary vascular remodelling that drives PAH. Osteoprotegerin (OPG) is increased within serum and lesions of patients with idiopathic PAH and is a mitogen and migratory stimulus for pulmonary artery smooth muscle cells (PASMCs). Here, we report that the pro-proliferative and migratory phenotype in PASMCs stimulated with OPG is mediated via the Fas receptor and that treatment with a human antibody targeting OPG can attenuate pulmonary vascular remodelling associated with PAH in multiple rodent models of early and late treatment. We also demonstrate that the therapeutic efficacy of the anti-OPG antibody approach in the presence of standard of care vasodilator therapy is mediated by a reduction in pulmonary vascular remodelling. Targeting OPG with a therapeutic antibody is a potential treatment strategy in PAH.
Conflict of interest statement
A.L./The University of Sheffield has been granted intellectual property around the area of targeting OPG for the treatment of PAH (GB2510524 / US9334327 / JP2014532637) and is a founding Director of PH Therapeutics Ltd, a University of Sheffield Spin-out company. J.C., V.G., M.M. and P.B.-W. are employees of Kymab Ltd and hold share options in the company. Kymab has filed intellectual property (GB1701416.8) around the characteristics of a therapeutic human anti-osteoprotegerin antibody with A.L. named as an inventor. The remaining authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
- FS/08/061/25740/BHF_/British Heart Foundation/United Kingdom
- G0800318/MRC_/Medical Research Council/United Kingdom
- MR/L023040/1/MRC_/Medical Research Council/United Kingdom
- FS/13/48/30453/British Heart Foundation (BHF)/International
- FS/18/13/33281/BHF_/British Heart Foundation/United Kingdom
- FS/13/48/30453/BHF_/British Heart Foundation/United Kingdom
- FS/18/52/33808/British Heart Foundation (BHF)/International
- MC_PC_12022/MRC_/Medical Research Council/United Kingdom
- FS/18/52/33808/BHF_/British Heart Foundation/United Kingdom
- 206632/Z/17/Z/Wellcome Trust (Wellcome)/International
- MR/K002406/1/RCUK | Medical Research Council (MRC)/International
- FS/08/061/25740/British Heart Foundation (BHF)/International
- 206632/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- MR/K002406/1/MRC_/Medical Research Council/United Kingdom
- CH/09/001/25945/BHF_/British Heart Foundation/United Kingdom
- FS/18/13/33281/British Heart Foundation (BHF)/International
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
