

A rationale for surgical debulking to improve anti-PD1 therapy outcome in non small cell lung cancer
- PMID: 31729430
- PMCID: PMC6858444
- DOI: 10.1038/s41598-019-52913-z
A rationale for surgical debulking to improve anti-PD1 therapy outcome in non small cell lung cancer
Abstract
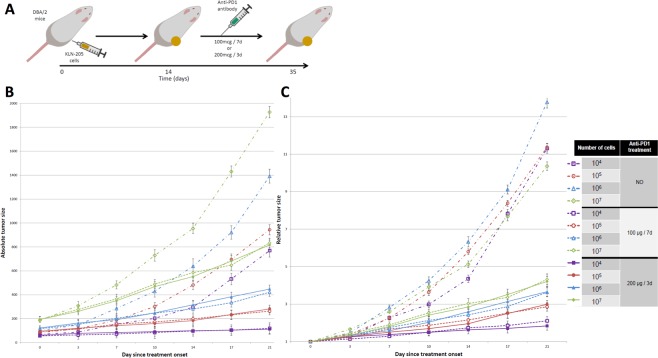
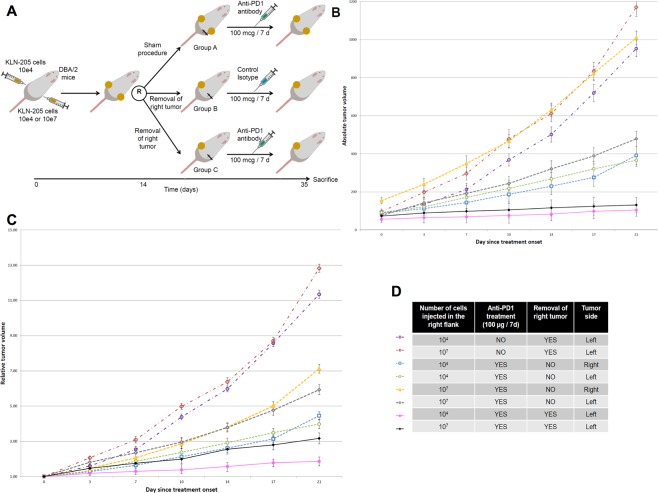
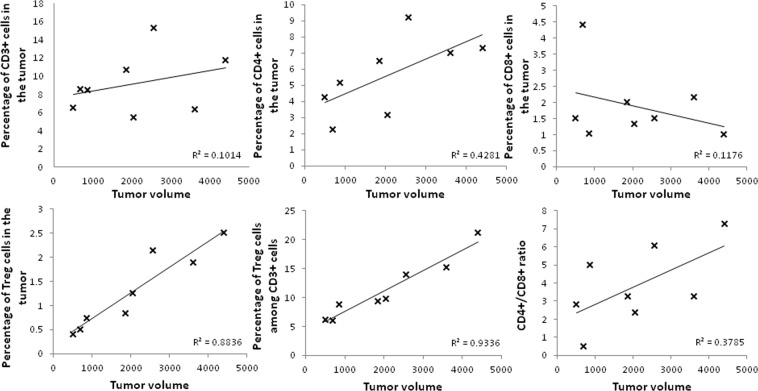
Anti-PD1 immunotherapy has emerged as a gold-standard treatment for first- or second-line treatment of stage IV NSCLC, with response rates ranging from 10 to 60%. Strategies to improve the disease control rate are needed. Several reports suggested that debulking surgery enhances anti-tumor immunity. We aimed at examining tumor burden as a predictive factor of anti-PD1 tretment efficacy and to evaluate the role of cytoreductive surgery in anti-PD1 treated NSCLC. Immunocompetent DBA/2 mice engrafted with various amount of allogeneic lung squamous cancer KLN-205 cells were treated with anti-PD1 monoclonal antibody. Mice engrafted with two tumors also underwent a debulking surgery or a sham procedure. Tumor volume was monitored to assess treatment efficacy. Tumor infiltrating lymphocytes were assessed by flow cytometry. In a retrospective study of 48 stage IV NSCLC patients treated with Nivolumab who underwent a 18-FDG PETscan before treatment onset, the prognostic role of metabolic tumor volume was analysed. Anti-PD1 treatment effect was greater in mice bearing smaller tumors. Treatment with higher doses of anti-PD1 antibody did not improve the outcome, independently of the size of the tumor. In mice bearing 2 tumors, excision of 1 tumor improved the anti-PD1 treatment effect on the remaining tumor. In 48 NSCLC patients receiving anti-PD1 treatment, high metabolic tumor volume was associated with poor overall survival and the absence of clinical benefit. Treg infiltration, but not effector T cells, was positively correlated to tumor volume. Taken together, our results suggest that tumor volume is a predictive factor of anti-PD1 efficacy in NSCLC. Additionally, an experimental murine model suggests that tumor debulking may improve control of residual tumor.
Conflict of interest statement
F.G. reports personal fees from BMS, MSD/MERCK US, ASTRA ZENECA, BOEHRINGER INGELHEIM and ROCHE, and non-financial support from BMS, BOEHRINGER INGELHEIM, CHUGAI and PFIZER, outside the submitted work.
Figures
References
-
- Mickisch GH, Garin A, van Poppel H, de Prijck L, Sylvester R. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma: a randomised trial. Lancet (London, England) 2001;358:966–970. doi: 10.1016/S0140-6736(01)06103-7. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
