

Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors
- PMID: 31730012
- PMCID: PMC6858629
- DOI: 10.1186/s40425-019-0805-8
Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors
Abstract
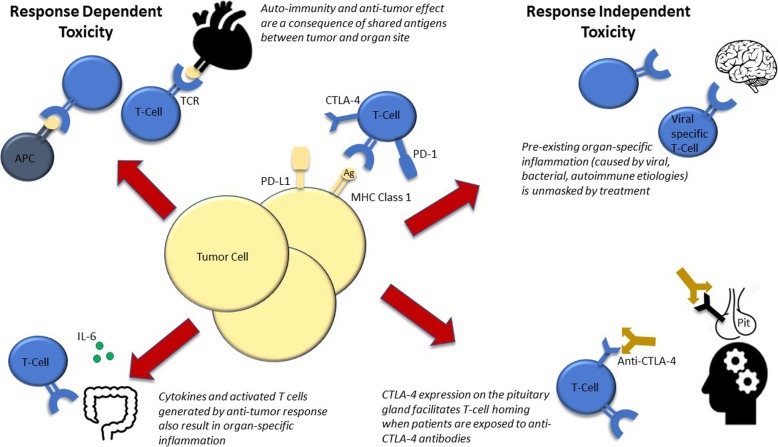
Although immune checkpoint inhibitors (ICIs) have transformed the treatment landscape for patients with many advanced malignancies, only 15-60% of patients respond, leaving a broad swath of patients who do not derive benefit. Identifying biomarkers to optimally identify patients who will benefit from ICIs is a major research focus for the oncology community. Thus far, predictive biomarker research has focused on tumor signatures such as microsatellite instability, programmed death-ligand 1 (PD-L1) expression and tumor mutational burden; clinical biomarkers have been far less studied. One potential clinical biomarker for ICI response in patients is immune-related adverse event (IRAE) onset.IRAEs are thought to represent bystander effects from activated T-cells and it is plausible that patients responding to ICIs would have greater likelihood of autoimmune toxicities (e.g. due to a more competent/treatment-responsive immune system, or cross-reactivity between tumor and host tissue). Earlier studies in melanoma patients however, suggested no association between IRAE onset and anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) antibody efficacy. In contrast, a growing body of literature suggests IRAE onset is predictive of anti-programmed cell death protein 1 (PD-1) and anti-PD-L1 antibody response across a variety of solid tumors. Most of these studies report that patients who experienced IRAEs demonstrate marked improvements in progression-free survival, overall survival and overall response rate compared to those lacking toxicity.Key questions regarding the association between IRAE onset and ICI efficacy remain. The most pertinent of these involve whether the association is only relevant for patients treated with anti-PD-1 and anti-PD-L1 antibodies and whether IRAE site, severity, timing of onset and management influence ICI efficacy. Herein, we discuss the seminal studies which have begun to address these questions and have shaped the narrative about the predictive value of IRAE onset for patients on ICIs, in this review.
Keywords: Anti-cytotoxic T-lymphocyte-associated protein 4; Anti-programmed cell death protein 1; Anti-programmed death-ligand 1; Autoimmunity and anti-tumor effect; Immune checkpoint inhibitor efficacy; Immune-related adverse events.
Conflict of interest statement
Dr. Johnson is on advisory boards for Array Biopharma, BMS, Incyte, Merck, and Novartis, receives research support from BMS and Incyte, and received travel support from Genentech.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials