

Review
doi: 10.1530/ERP-19-0048.
Online ahead of print.
EDUCATIONAL SERIES IN CONGENITAL HEART DISEASE: Cardiovascular MRI and CT in congenital heart disease
Affiliations
- PMID: 31730044
- PMCID: PMC6893312
- DOI: 10.1530/ERP-19-0048
Item in Clipboard
Review
EDUCATIONAL SERIES IN CONGENITAL HEART DISEASE: Cardiovascular MRI and CT in congenital heart disease
Echo Res Pract.
.
Abstract
Cardiovascular MRI and CT are useful imaging modalities complimentary to echocardiography. This review article describes the common indications and consideration for the use of MRI and CT in the management of congenital heart disease.
Figures

Balanced SSFP cine imaging in a patient with a dilated RVOT, pulmonary regurgitation and dilated RV post repair of tetralogy of Fallot (Video 1).
Two-dimensional black blood images of the right and left pulmonary arteries.
Contrast-enhanced MR angiography of the right ventricle and branch pulmonary arteries, and the pulmonary veins, left ventricle and aorta.
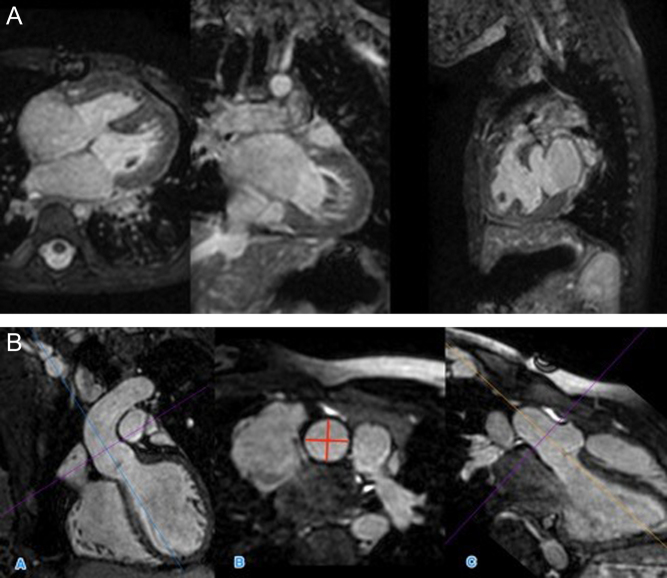
(A) 3D SSFP dataset, in coronal, axial and sagittal planes. (B) MPR of 3D SFFP image demonstrating measurement of the sinotubular junction of the aorta. This is measured in image B, from orthogonal planes (A and C).
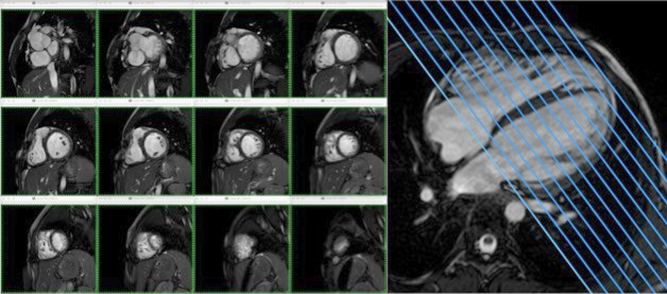
Ventricular volumes are generated from a stack of 2D cine CMR slices across the ventricle.
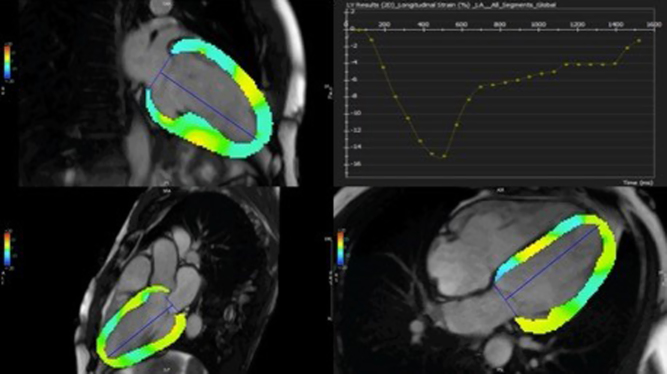
CMRFT quantifying global longitudinal strain of the left ventricle.
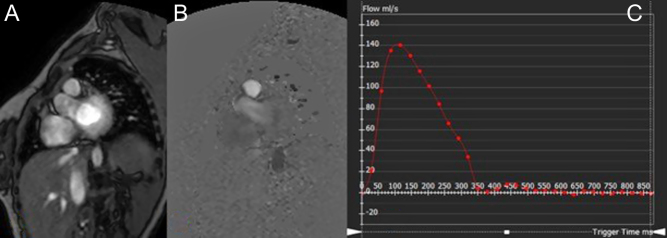
Magnitude (A) and phase-contrast flow images (B) and flow map measurement using MR analysis software (C) (in this case the main pulmonary artery). The flow value is the area under the curve.
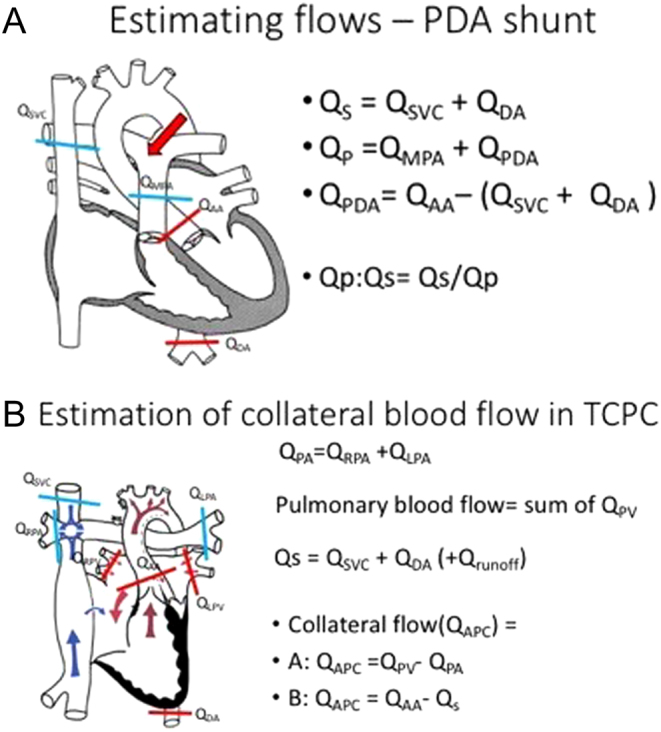
(A) Estimation of flow from a PDA. (B) Estimation of aortopulmonary Collateral flow in a Fontan.
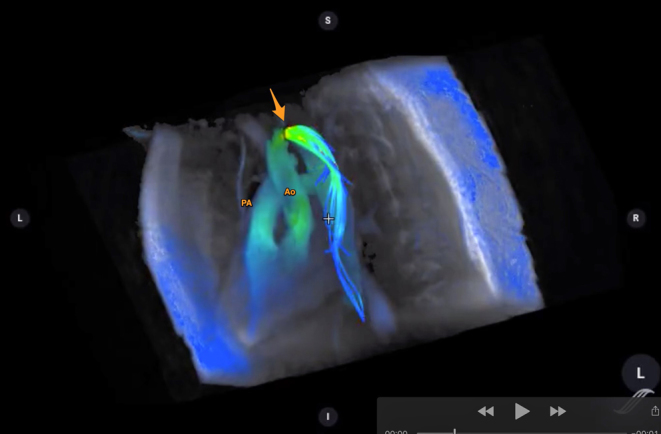
4D flow image of a patient with coarctation of aorta. The great vessels (pulmonary artery, PA and aorta, Ao) are annotated. The arrow points towards the coarctation. Flow acceleration is denoted in the flow velocity colour map as shown. (Image courtesy of Dr Francesca Raimondi, Hôpital Universitaire Necker – Enfants Malades, Paris, France.)
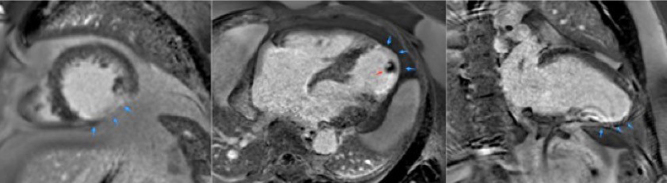
Late gadolinium enhancement images (LGE) of apical short axis, four-chamber and two-chamber view. LGE in the mid and apical inferior aspect of the LV. Infarcted area shows delayed gadolinium uptake (blue arrows pointing at the bright white structure). In this instance the effect is transmural. This corresponds to an invasive coronary angiogram finding of a thrombosed distal left anterior descending artery. The apical thrombus is also shown (red arrow).
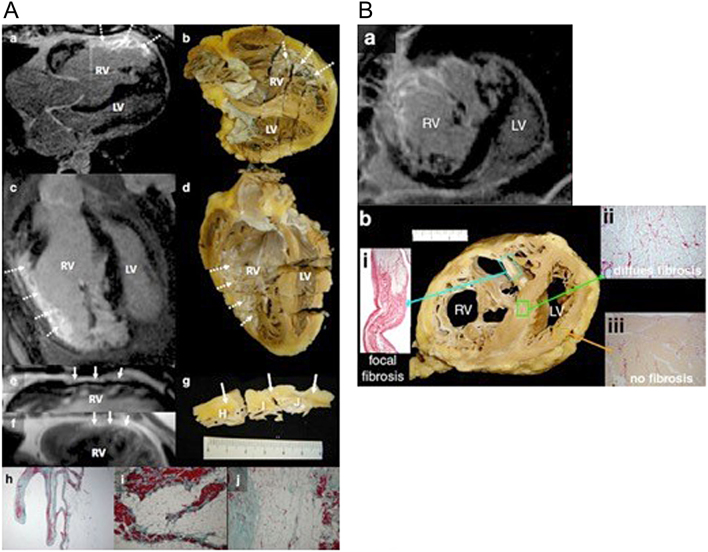
Macroscopic fibrosis and correlation with in vivo late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) in heart explanted during follow-up. LGE CMR (A and C) and corresponding photographs of macroscopic sections (B and D) showing excellent correlation of CMR LGE with visually fibrotic areas (arrows). The increased signal on balanced steady state free precession (E) and turbo spin echo (F; continuous arrows) is compatible with fat. In (G), the corresponding macroscopic specimen shows epicardial fatty infiltration (continuous arrows) but also right ventricular (RV) endocardial fibrosis. Corresponding histology is shown after staining with Masson’s Trichrome; region (H) shows extensive replacement of the compact myocardium by fatty tissue, whereas the trabeculations lining the cavity contain myocardium (red) and extensive fibrous tissue (green, ×16). Regions (I) and (J) show extensive fatty and fibrous replacement (×100). (B) Microscopic fibrosis and correlation with in vivo LGE CMR. Extensive RV LGE (A; short axis CMR plane) corresponded with macroscopic fibrosis in the explanted heart (B; transverse specimen) with Picrosirius Red staining confirmed collagen in the area of macroscopic fibrosis and corresponding LGE (i inset). Apparently normal looking myocardium at ×25 magnification (ii) shows a lower degree of interstitial/diffuse fibrosis undetected by LGE CMR. No fibrosis was detected in the subpulmonary LV (iii) (22).
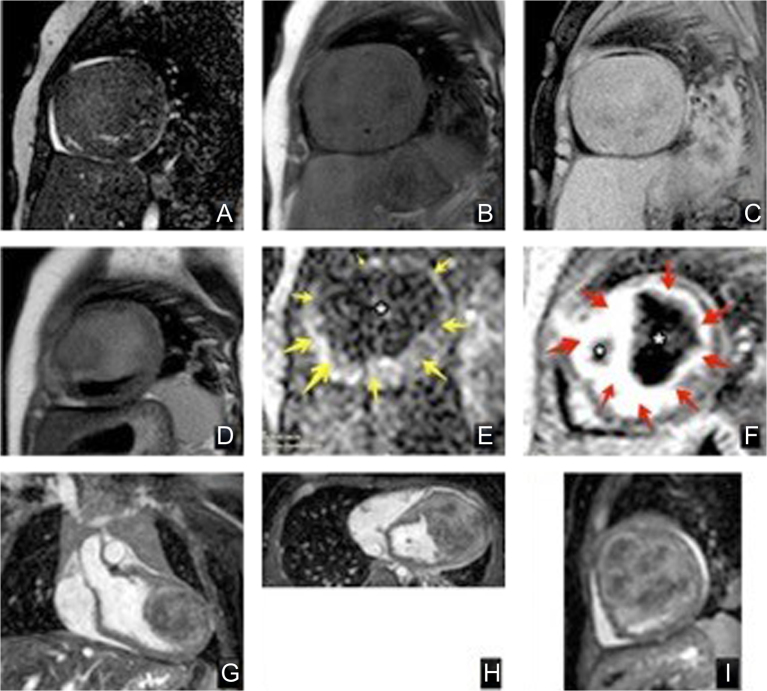
Tumour characterisation using different MR techniques, of a cardiac fibroma. Top row: (A) 2D balanced SSFP cine iso-intense signal with the myocardium, (B) T1 black blood with no fat suppression showing heterogenous texture with hyper-intense signal of the tumour capsule compared to myocardium and skeletal muscle, and (C) T1 black blood with fat suppression suggests that the tumour is not comprised of fatty tissue. Middle row: (D) T2 turbo-spin-echo black blood, (E) first pass perfusion image with no enhancement of the tumour (dark, *) compared to normal myocardium (yellow arrows) suggesting a non-vascular nature, and (F), late gadolinium enhancement, with high signal (red arrows) with a low signal dark core (*). Bottom row: multiplanar reconstruction using 3D SSFP dataset to locate extent of the tumour within the heart. Coronal (G), axial (H) and sagittal (I) view of the heart with location of the cardiac tumour.
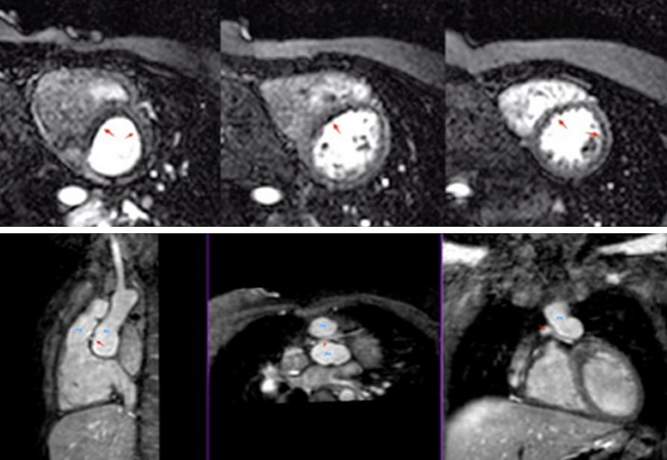
Patient with transposition of great arteries post arterial switch operation and retro-pulmonary left coronary artery, presented with chest pain on exertion. Normal systolic function at rest. However, on stress perfusion, the images reveal perfusion defects in the left anterior descending artery and circumflex territories. Lower row images show relationship between the pulmonary artery (PA), aorta (Ao) and left main coronary artery (red arrow) (Video 5).
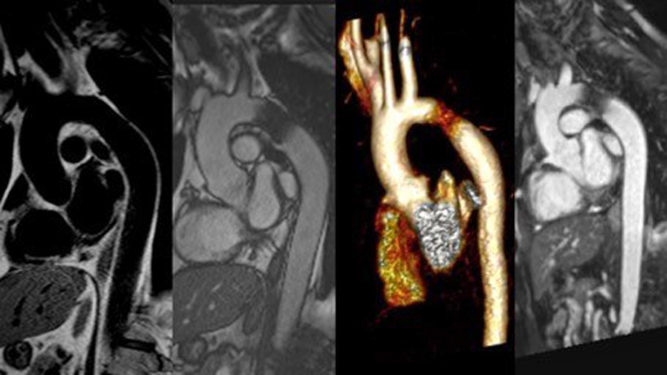
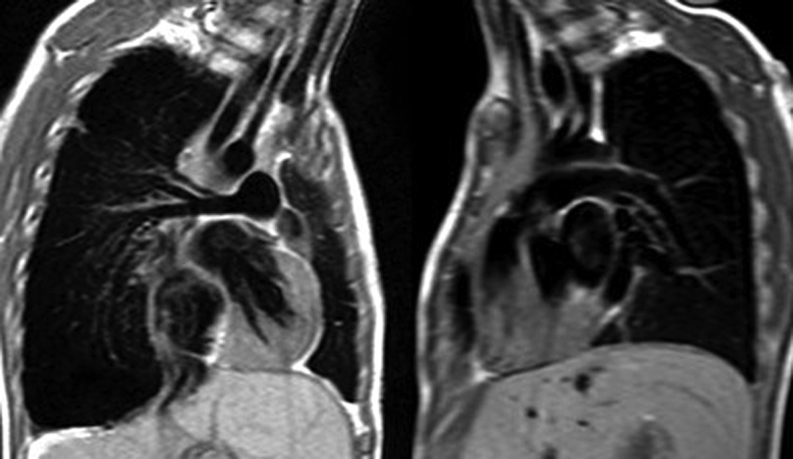
A case of coarctation of aorta following stent implantation. Different MRI techniques shown to investigate the intervened vascular structure. From left to right are black-blood, balanced SSFP cine, volume-rendered MR angiography and a multiplanar reconstruction from a 3-dimensional SSFP (3D whole heart) dataset.
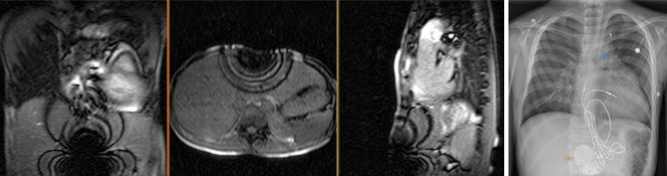
Artefacts from metal objects in MRI. This 11-year-old boy had MRI–conditional pacemaker and pacing leads (Medtronic SureScan) system and a left pulmonary artery stent in situ. Images 1, 2 and 3 represent the coronal, axial and sagittal views from the MRI survey. Image 4 is a chest X-ray of the same patient prior to MRI scan. The MRI-conditional pacemaker box (orange arrow) and left pulmonary artery stent (blue arrow) are shown.
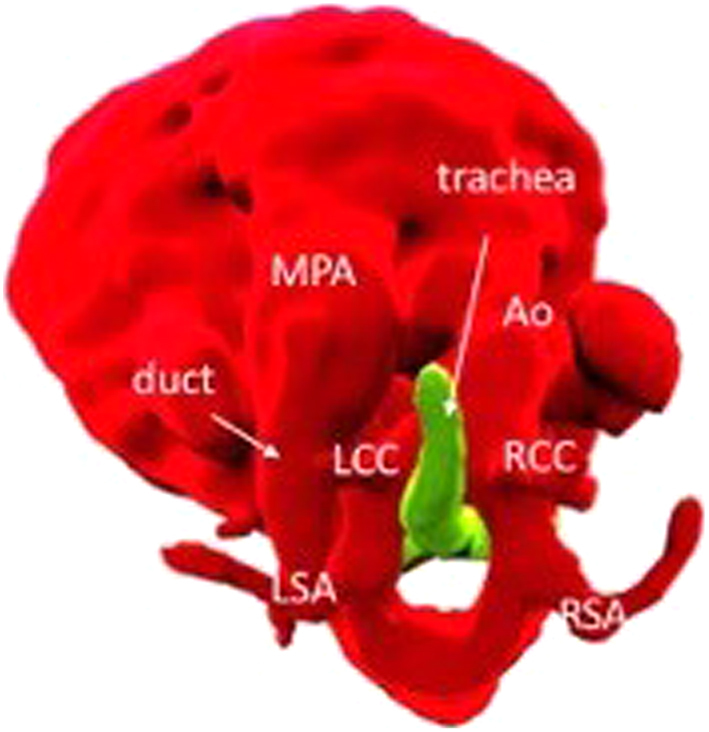
Volume-rendered view of a double aortic arch from a fetal CMR at 30 + 4 weeks gestation.
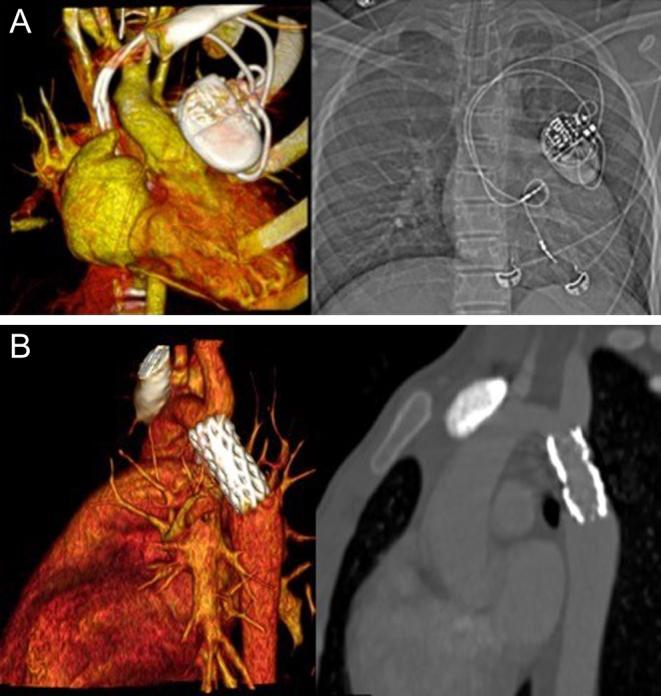
(A) Volume-rendered image of a pacemaker on a CT angiogram, paired with a plain CXR on the right. (B) Contrast-enhanced CT images showing volume rendered (left) and multiplanar reconstruction (MPR) (right) post coarctation stent.
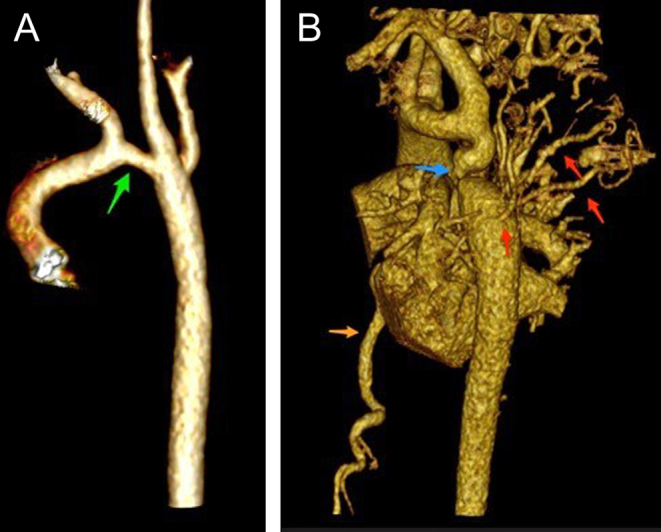
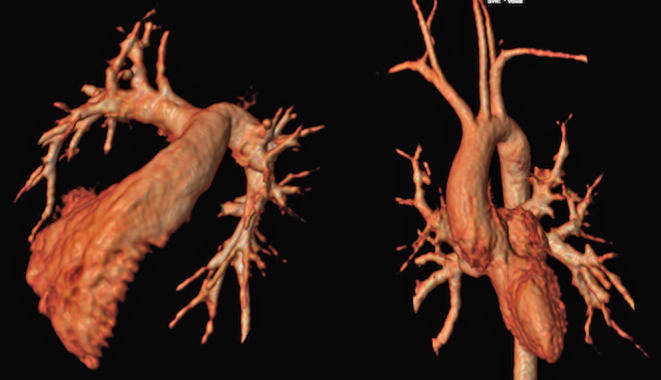
Volume-rendered images of aortic arch. Image (A) (to the left) was aortic arch of an infant following surgical repair, with residual transverse arch hypoplasia (green arrow). Image (B) (to the right) shows a case of coarctation in an older child (12 years). There is transverse arch hypoplasia, tortuous isthmus with coarctation (blue arrow). There is post-coarctation dilatation. Extensive network of thoracic collateral vessels (red arrows) and dilated intermammary arteries (orange arrow).

Contrast-enhanced CT of pulmonary atresia, ventricular septal defect and MAPCA (major aortopulmonary collateral arteries) and right-sided aortic arch. The main pulmonary artery has been anastomosed with a classic central shunt created by the left subclavian artery. This patient has been unifocalised, with some residual MAPCAS. The study was done to assess anatomy prior to RV-PA conduit reconstruction.
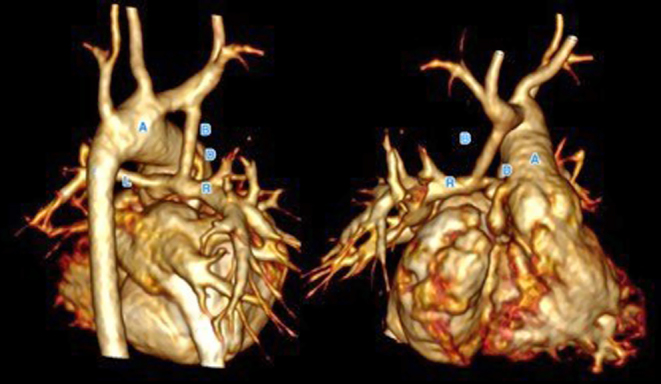
Contrast-enhanced rendered volume of a patent with hypoplastic left heart syndrome following Norwood stage I with right modified BT shunt. The shunt (B) is patent and anastomosed to the right pulmonary artery (R). The left pulmonary artery (L) is slender. The reconstructed aortic arch (A) and Damus Kaye Stansel (D) anastomosis is patent.
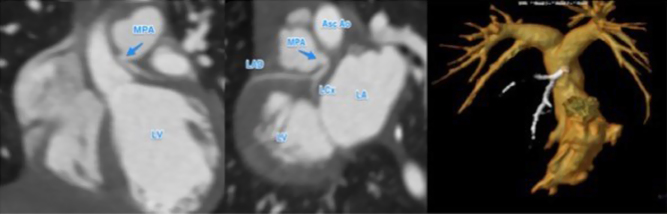
Anomalous left coronary artery arising from the main pulmonary artery (MPA). The left coronary artery does not arise from the aortic root (left hand image). The left coronary ostium is traced back to the MPA. This gives rise to the left anterior descending artery (LAD) and left circumflex (LCx). The left ventricle (LV) and left atrium (LA) are dilated, in association with impaired ventricular function prior to surgery. The right-hand image shows a volume rendered view of the right ventricle, MPA and branch pulmonary arteries (yellow). The left coronary artery (white) arise for the MPA.
References
-
- Valente AM, Cook S, Festa P, Ko HH, Krishnamurthy R, Taylor AM, Warnes CA, Kreutzer J, Geva T. Multimodality imaging guidelines for patients with repaired tetralogy of Fallot: a report from the American Society of Echocardiography: developed in collaboration with the Society for Cardiovascular Magnetic Resonance and the Society for Pediatric Radiology. Journal of the American Society of Echocardiography 2014. 111–141. (10.1016/j.echo.2013.11.009) - DOI - PubMed
-
- Cohen MS, Eidem BW, Cetta F, Fogel MA, Frommelt PC, Ganame J, Han BK, Kimball TR, Johnson RK, Mertens L, et al. Multimodality imaging guidelines of patients with transposition of the great arteries: a report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance and the Society of Cardiovascular Computed Tomography. Journal of the American Society of Echocardiography 2016. 571–621. (10.1016/j.echo.2016.04.002) - DOI - PubMed
-
- Di Salvo G, Miller O, Babu Narayan S, Li W, Budts W, Valsangiacomo Buechel ER, Frigiola A, van den Bosch AE, Bonello B, Mertens L, et al. Imaging the adult with congenital heart disease: a multimodality imaging approach-position paper from the EACVI. European Heart Journal: Cardiovascular Imaging 2018. 1077–1098. (10.1093/ehjci/jey102) - DOI - PubMed
-
- Luijnenburg SE, Robbers-Visser D, Moelker A, Vliegen HW, Mulder BJ, Helbing WA. Intra-observer and interobserver variability of biventricular function, volumes and mass in patients with congenital heart disease measured by CMR imaging. International Journal of Cardiovascular Imaging 2010. 57–64. (10.1007/s10554-009-9501-y) - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
