

Self-monitoring of Blood Pressure in Patients With Hypertension-Related Multi-morbidity: Systematic Review and Individual Patient Data Meta-analysis
- PMID: 31730171
- PMCID: PMC7162426
- DOI: 10.1093/ajh/hpz182
Self-monitoring of Blood Pressure in Patients With Hypertension-Related Multi-morbidity: Systematic Review and Individual Patient Data Meta-analysis
Abstract
Background: Studies have shown that self-monitoring of blood pressure (BP) is effective when combined with co-interventions, but its efficacy varies in the presence of some co-morbidities. This study examined whether self-monitoring can reduce clinic BP in patients with hypertension-related co-morbidity.
Methods: A systematic review was conducted of articles published in Medline, Embase, and the Cochrane Library up to January 2018. Randomized controlled trials of self-monitoring of BP were selected and individual patient data (IPD) were requested. Contributing studies were prospectively categorized by whether they examined a low/high-intensity co-intervention. Change in BP and likelihood of uncontrolled BP at 12 months were examined according to number and type of hypertension-related co-morbidity in a one-stage IPD meta-analysis.
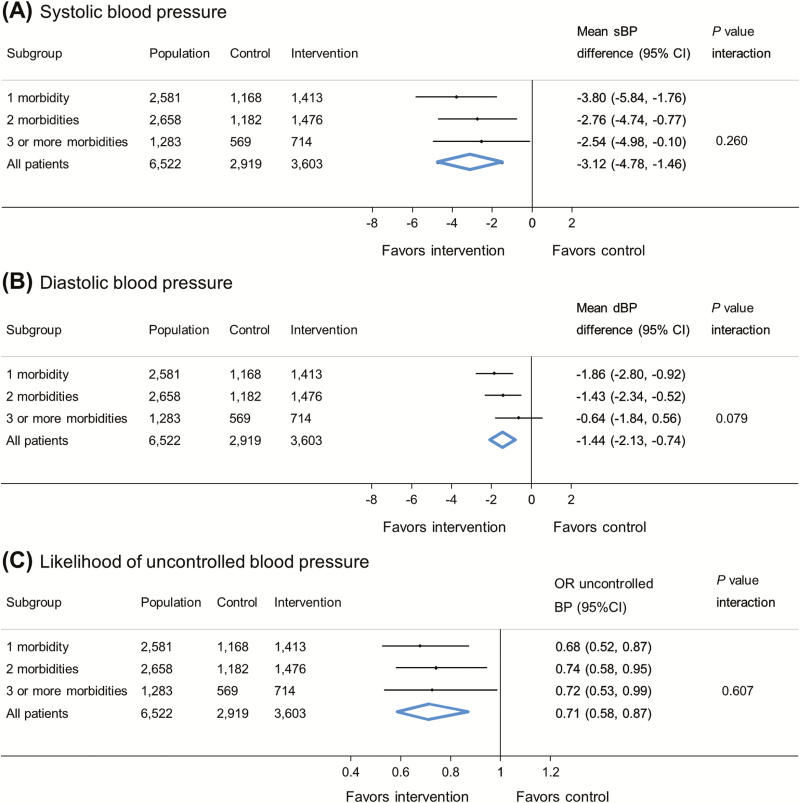
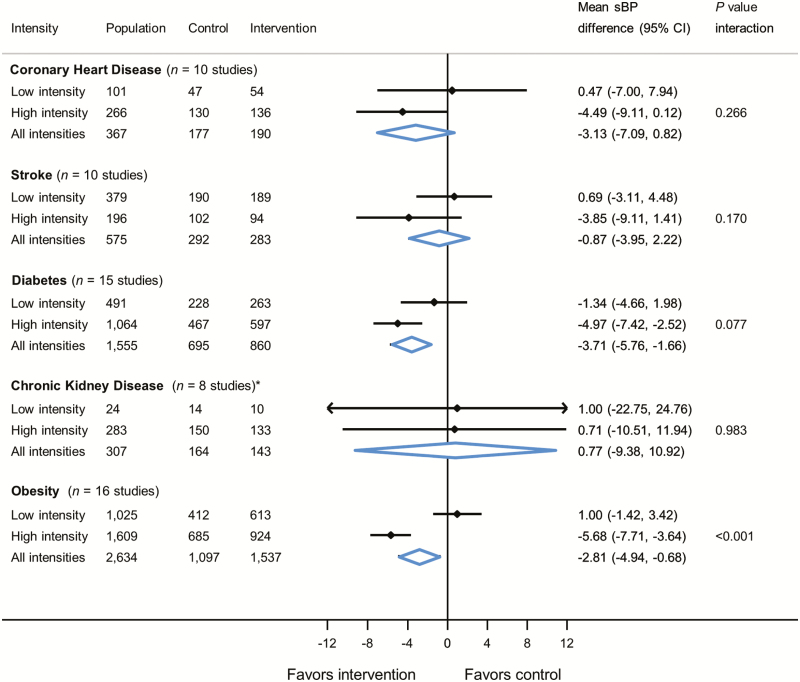
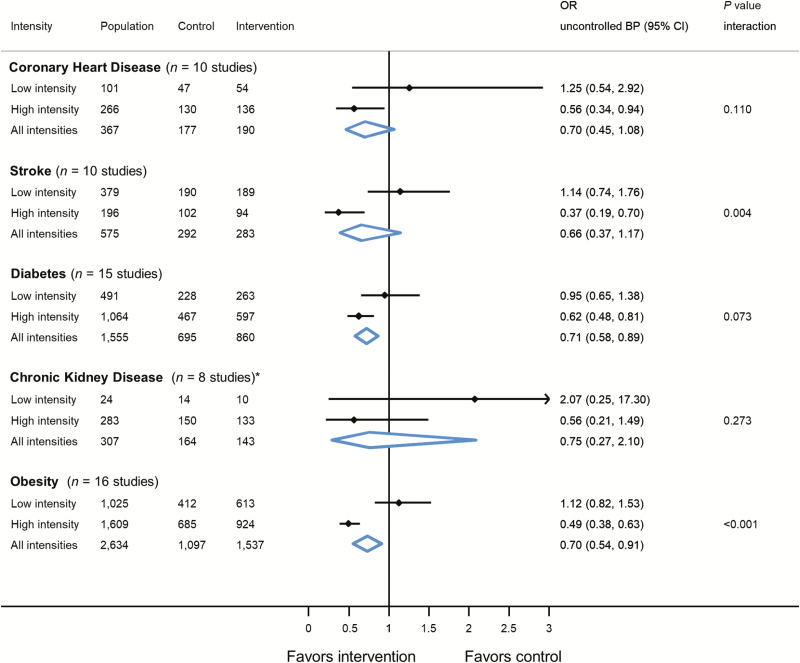
Results: A total of 22 trials were eligible, 16 of which were able to provide IPD for the primary outcome, including 6,522 (89%) participants with follow-up data. Self-monitoring was associated with reduced clinic systolic BP compared to usual care at 12-month follow-up, regardless of the number of hypertension-related co-morbidities (-3.12 mm Hg, [95% confidence intervals -4.78, -1.46 mm Hg]; P value for interaction with number of morbidities = 0.260). Intense interventions were more effective than low-intensity interventions in patients with obesity (P < 0.001 for all outcomes), and possibly stroke (P < 0.004 for BP control outcome only), but this effect was not observed in patients with coronary heart disease, diabetes, or chronic kidney disease.
Conclusions: Self-monitoring lowers BP regardless of the number of hypertension-related co-morbidities, but may only be effective in conditions such obesity or stroke when combined with high-intensity co-interventions.
Keywords: blood pressure; coronary heart disease; diabetes; hypertension; obesity; randomized controlled trial; stroke.
© The Author(s) 2019. Published by Oxford University Press on behalf of American Journal of Hypertension, Ltd.
Figures
References
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet 2012; 380:37–43. - PubMed
-
- Wang HH, Wang JJ, Wong SY, Wong MC, Li FJ, Wang PX, Zhou ZH, Zhu CY, Griffiths SM, Mercer SW. Epidemiology of multimorbidity in China and implications for the healthcare system: cross-sectional survey among 162,464 community household residents in southern China. BMC Med 2014; 12:188. - PMC - PubMed
-
- Ornstein SM, Nietert PJ, Jenkins RG, Litvin CB. The prevalence of chronic diseases and multimorbidity in primary care practice: a PPRNet report. J Am Board Fam Med 2013; 26:518–524. - PubMed
-
- Violán C, Foguet-Boreu Q, Roso-Llorach A, Rodriguez-Blanco T, Pons-Vigués M, Pujol-Ribera E, Muñoz-Pérez MÁ, Valderas JM. Burden of multimorbidity, socioeconomic status and use of health services across stages of life in urban areas: a cross-sectional study. BMC Public Health 2014; 14:530. - PMC - PubMed
