

Aging and Lung Disease
- PMID: 31730381
- PMCID: PMC7998901
- DOI: 10.1146/annurev-physiol-021119-034610
Aging and Lung Disease
Abstract
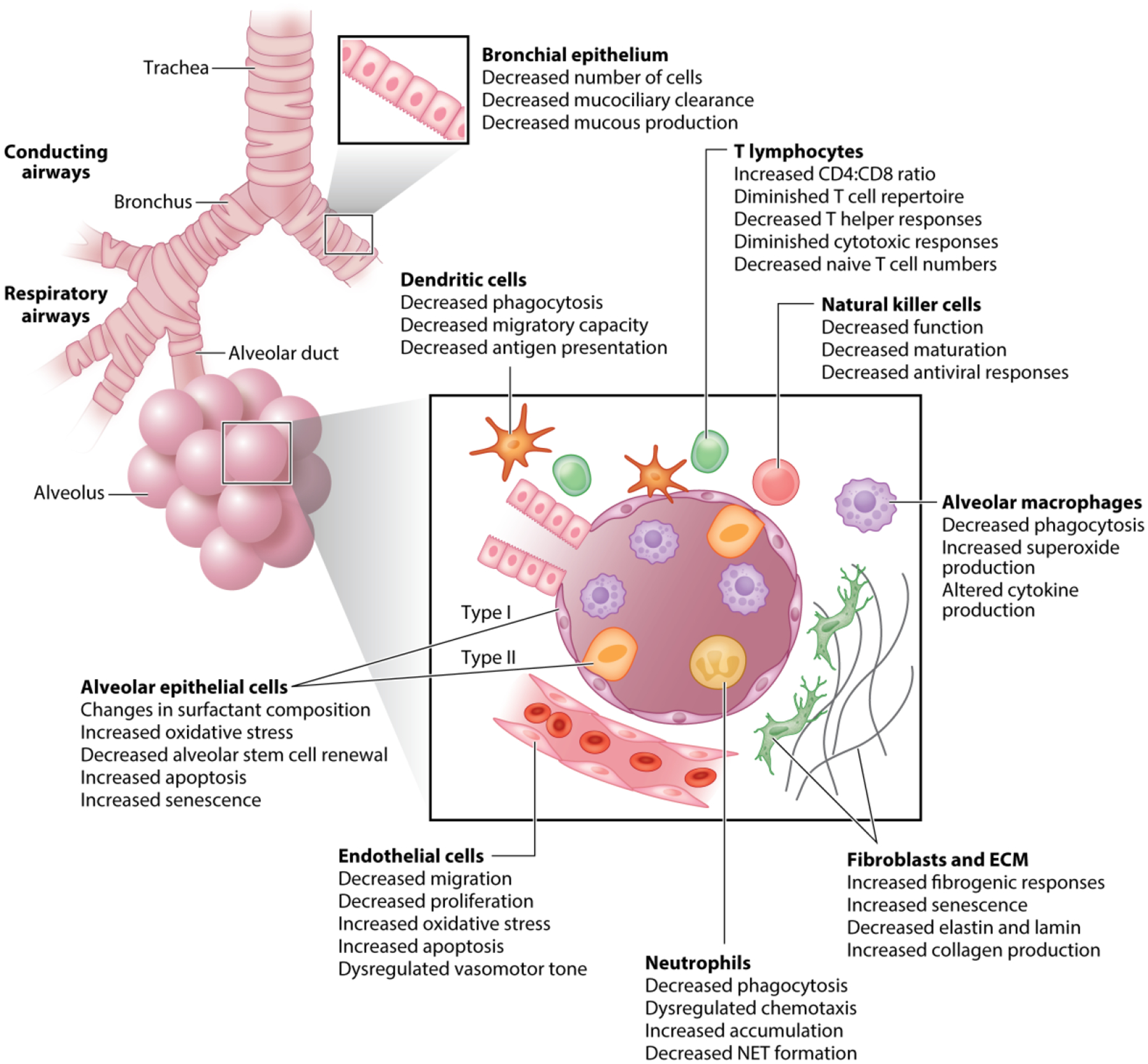
People worldwide are living longer, and it is estimated that by 2050, the proportion of the world's population over 60 years of age will nearly double. Natural lung aging is associated with molecular and physiological changes that cause alterations in lung function, diminished pulmonary remodeling and regenerative capacity, and increased susceptibility to acute and chronic lung diseases. As the aging population rapidly grows, it is essential to examine how alterations in cellular function and cell-to-cell interactions of pulmonary resident cells and systemic immune cells contribute to a higher risk of increased susceptibility to infection and development of chronic diseases, such as chronic obstructive pulmonary disease and interstitial pulmonary fibrosis. This review provides an overview of physiological, structural, and cellular changes in the aging lung and immune system that facilitate the development and progression of disease.
Keywords: ARDS; COPD; IPF; acute respiratory distress syndrome; chronic obstructive pulmonary disease; inflammation; interstitial pulmonary fibrosis; lung aging; pneumonia.
Figures


References
-
- Beaty TH, Cohen BH, Newill CA, Menkes HA, Diamond EL, Chen CJ. 1982. Impaired pulmonary function as a risk factor for mortality. Am. J. Epidemiol 116:102–13 - PubMed
-
- Liu D, Hornsby PJ. 2007. Senescent human fibroblasts increase the early growth of xenograft tumors via matrix metalloproteinase secretion. Cancer Res. 67:3117–26 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
