

STAT3: An Emerging Therapeutic Target for Hepatocellular Carcinoma
- PMID: 31731457
- PMCID: PMC6895841
- DOI: 10.3390/cancers11111646
STAT3: An Emerging Therapeutic Target for Hepatocellular Carcinoma
Abstract
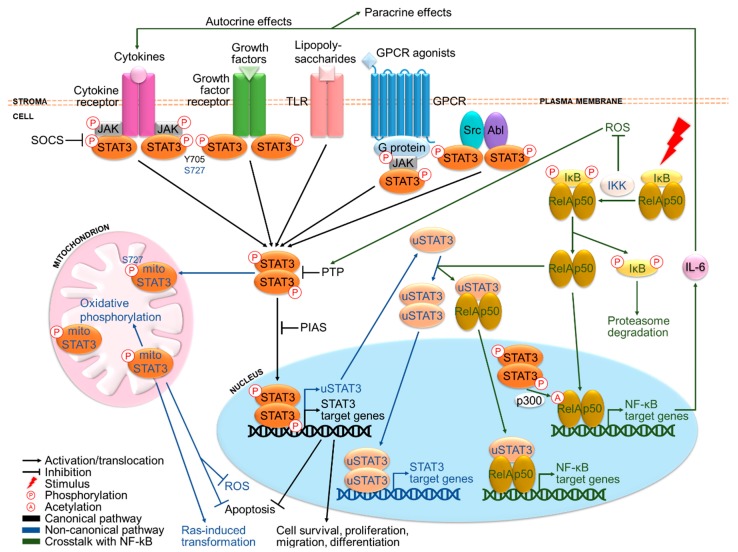
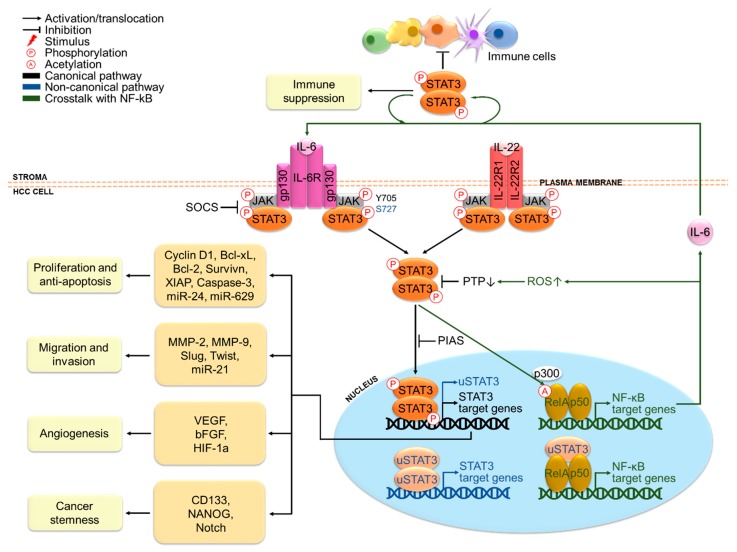
Hepatocellular carcinoma (HCC) is a major global health problem and its treatment options have been limited. Signal transducer and activator of transcription 3 (STAT3) is a transcription factor important for various cellular processes. Overexpression and constitutive activation of STAT3 have been frequently found in HCC and associated with poor prognosis. Ample evidence has shown that STAT3 plays pivotal roles in the initiation, progression, metastasis and immune suppression of HCC. Thus, STAT3 has attracted attention as a novel therapeutic target in HCC. Clinical trials have investigated STAT3-targeted therapeutics either as monotherapy or in combination with chemotherapeutic agents, immune checkpoint inhibitors and alternative targeted drugs. Some of these studies have yielded encouraging results. Particularly, napabucasin-a cancer stemness inhibitor targeting STAT3-driven gene transcription-has stood out with its promising clinical efficacy and safety profile. Nonetheless, clinical investigations of STAT3-targeted therapies in HCC are limited and more efforts are strongly urged to evaluate their clinical performance in HCC. Here, we provide a comprehensive review of the roles of STAT3 in HCC and follow by comprehensive analysis of STAT3 targeted strategies.
Keywords: STAT3; combination therapy; hepatocellular carcinoma; targeted therapy; transcription factor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- World Health Organization . GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012 v1.0. World Health Organization; Geneva, Switzerland: 2012.
-
- Imamura H., Matsuyama Y., Tanaka E., Ohkubo T., Hasegawa K., Miyagawa S., Sugawara Y., Minagawa M., Takayama T., Kawasaki S., et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J. Hepatol. 2003;38:200–207. doi: 10.1016/S0168-8278(02)00360-4. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
