

Tissue-Specific Macrophage Responses to Remote Injury Impact the Outcome of Subsequent Local Immune Challenge
- PMID: 31732166
- PMCID: PMC6892583
- DOI: 10.1016/j.immuni.2019.10.010
Tissue-Specific Macrophage Responses to Remote Injury Impact the Outcome of Subsequent Local Immune Challenge
Abstract
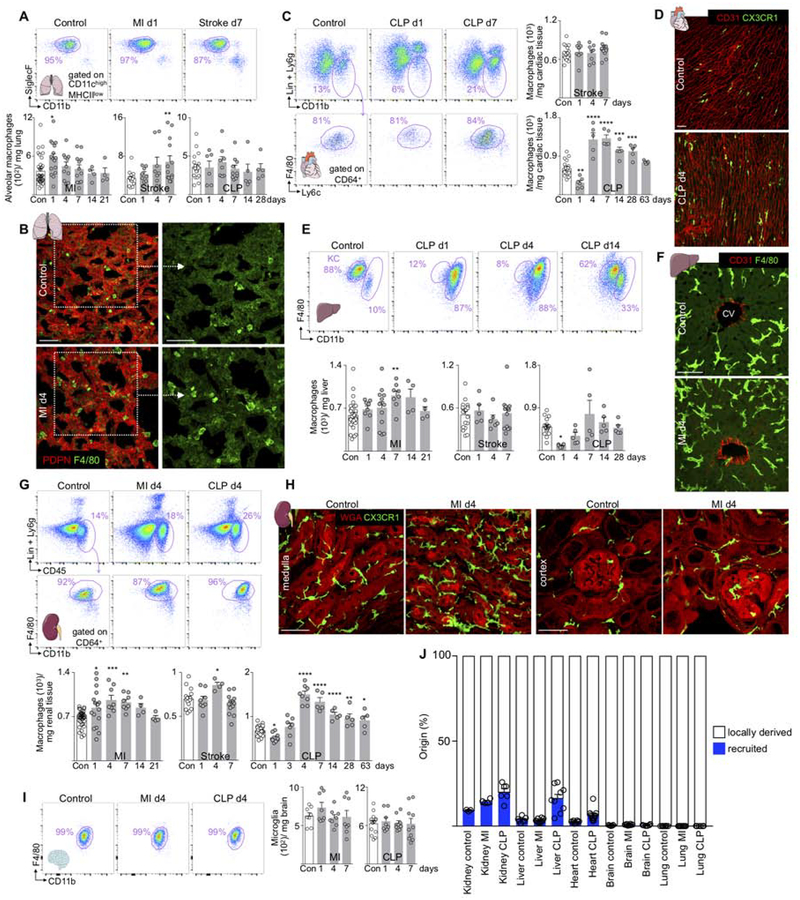
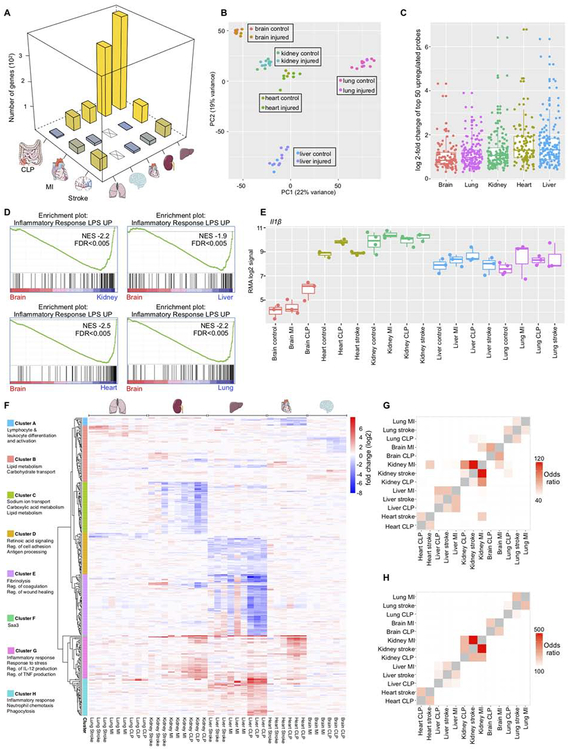
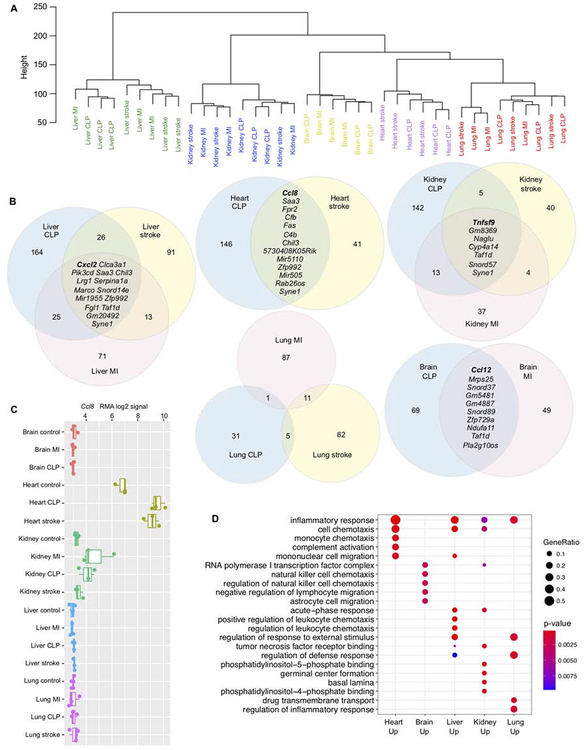
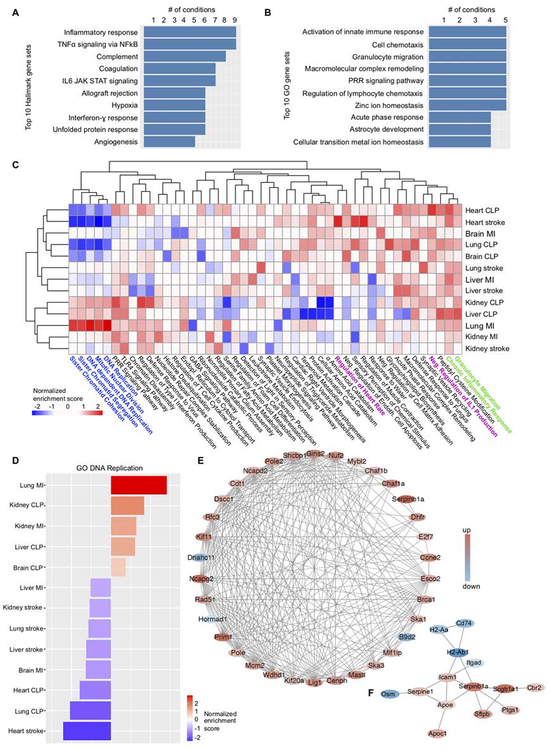
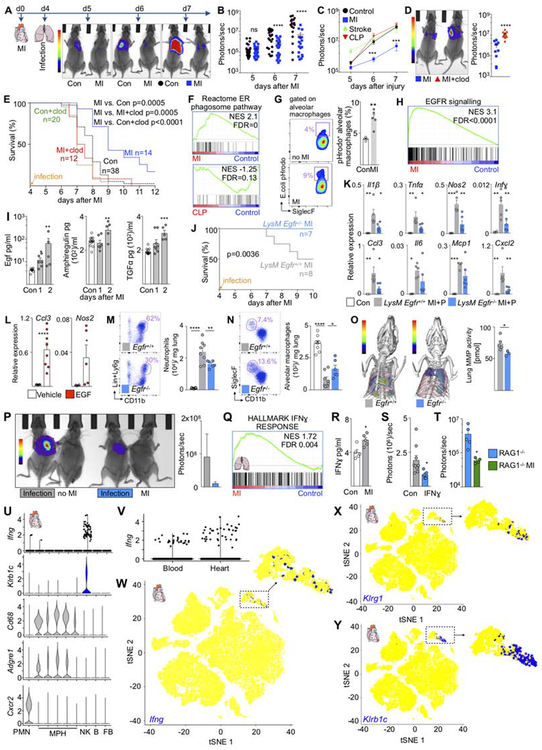
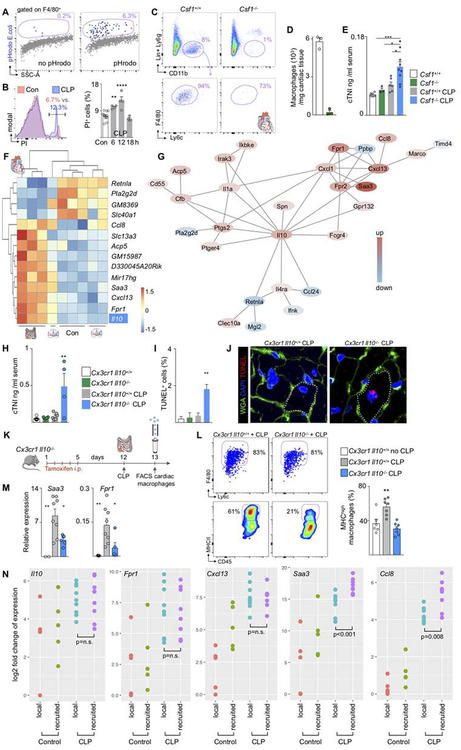
Myocardial infarction, stroke, and sepsis trigger systemic inflammation and organism-wide complications that are difficult to manage. Here, we examined the contribution of macrophages residing in vital organs to the systemic response after these injuries. We generated a comprehensive catalog of changes in macrophage number, origin, and gene expression in the heart, brain, liver, kidney, and lung of mice with myocardial infarction, stroke, or sepsis. Predominantly fueled by heightened local proliferation, tissue macrophage numbers increased systemically. Macrophages in the same organ responded similarly to different injuries by altering expression of tissue-specific gene sets. Preceding myocardial infarction improved survival of subsequent pneumonia due to enhanced bacterial clearance, which was caused by IFNɣ priming of alveolar macrophages. Conversely, EGF receptor signaling in macrophages exacerbated inflammatory lung injury. Our data suggest that local injury activates macrophages in remote organs and that targeting macrophages could improve resilience against systemic complications following myocardial infarction, stroke, and sepsis.
Keywords: macrophage; myocardial infarction; sepsis; stroke.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
DECLARATION OF INTERESTS
M.N. has been a paid a consultant fee or received research support from Alnylam, GSK, IFM Therapeutics, Medtronic, Molecular Imaging, Novartis, Sigilon and Verseaux.
Figures
Comment in
-
Macrophages react to remote challenges.Nat Rev Nephrol. 2020 Mar;16(3):132. doi: 10.1038/s41581-019-0236-2. Nat Rev Nephrol. 2020. PMID: 31776457 No abstract available.
References
-
- Chakarov S, Lim HY, Tan L, Lim SY, See P, Lum J, Zhang XM, Foo S, Nakamizo S, Duan K, Kong WT, Gentek R, Balachander A, Carbajo D, Bleriot C, Malleret B, Tam JKC, Baig S, Shabeer M, Toh SES, Schlitzer A, Larbi A, Marichal T, Malissen B, Chen J, Poidinger M, Kabashima K, Bajenoff M, Ng LG, Angeli V, and Ginhoux F (2019). Two distinct interstitial macrophage populations coexist across tissues in specific subtissular niches. Science 363, - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- DP2 AR075321/AR/NIAMS NIH HHS/United States
- R01 HL125428/HL/NHLBI NIH HHS/United States
- P30 DK043351/DK/NIDDK NIH HHS/United States
- K99 HL129168/HL/NHLBI NIH HHS/United States
- R01 GM083016/GM/NIGMS NIH HHS/United States
- R01 NS084863/NS/NINDS NIH HHS/United States
- P30 DK057521/DK/NIDDK NIH HHS/United States
- R01 GM053522/GM/NIGMS NIH HHS/United States
- R35 HL139598/HL/NHLBI NIH HHS/United States
- R01 GM119197/GM/NIGMS NIH HHS/United States
- T32 HL076136/HL/NHLBI NIH HHS/United States
- R01 HL128264/HL/NHLBI NIH HHS/United States
- UL1 TR001442/TR/NCATS NIH HHS/United States
- R37 CA225655/CA/NCI NIH HHS/United States
- P01 HL142494/HL/NHLBI NIH HHS/United States
- R00 HL129168/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
