

Cortical superficial siderosis and bleeding risk in cerebral amyloid angiopathy: A meta-analysis
- PMID: 31732564
- PMCID: PMC6937489
- DOI: 10.1212/WNL.0000000000008590
Cortical superficial siderosis and bleeding risk in cerebral amyloid angiopathy: A meta-analysis
Abstract
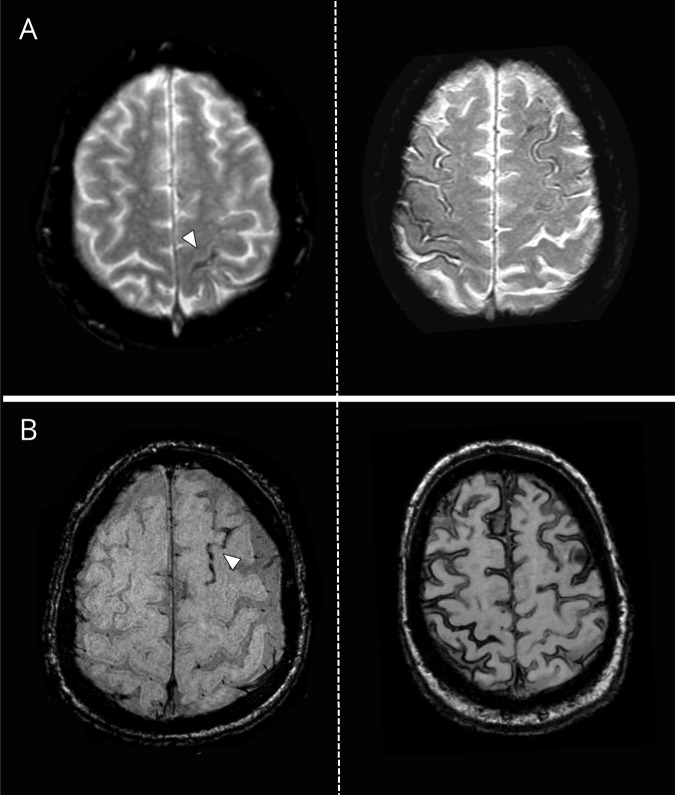
Objective: To assess the association of cortical superficial siderosis (cSS) presence and extent with future bleeding risk in cerebral amyloid angiopathy (CAA).
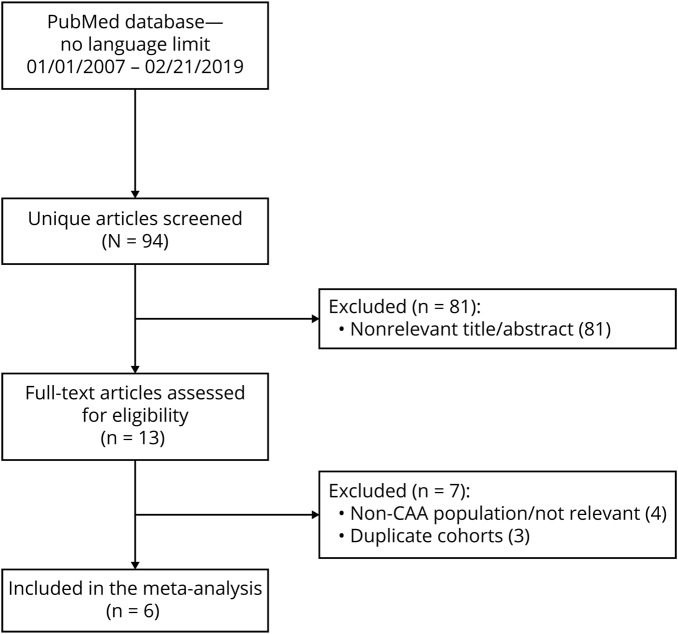
Methods: This was a meta-analysis of clinical cohorts of symptomatic patients with CAA who had T2*-MRI at baseline and clinical follow-up for future intracerebral hemorrhage (ICH). We pooled data in a 2-stage meta-analysis using random effects models. Covariate-adjusted hazard ratios (adjHR) from multivariable Cox proportional hazard models were used.
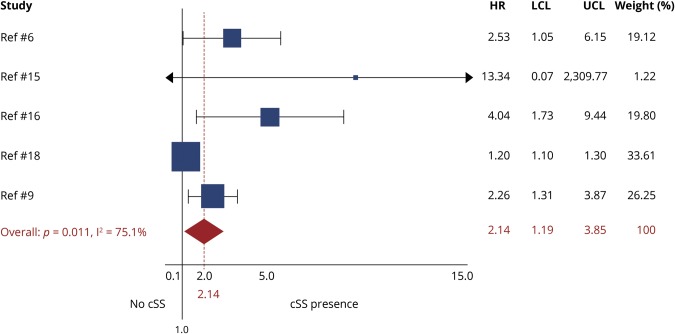
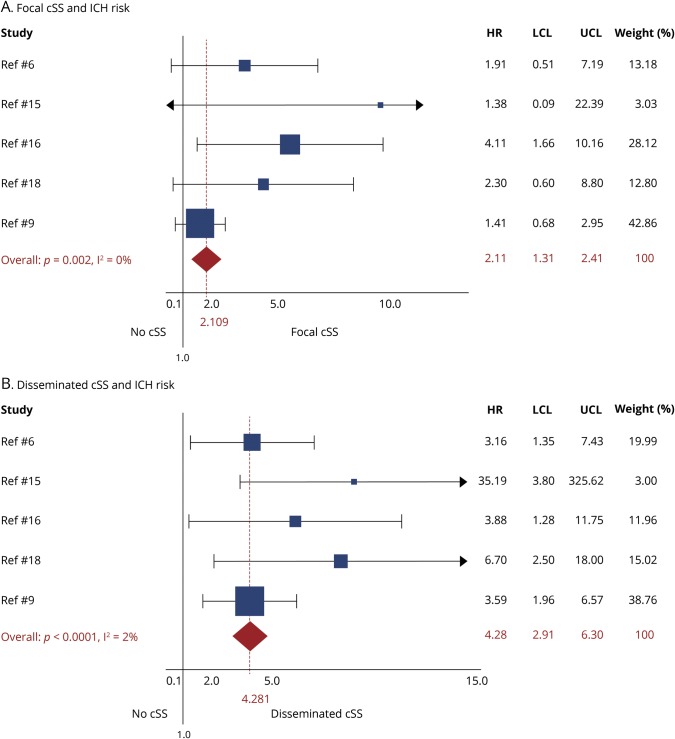
Results: We included data from 6 eligible studies (n = 1,239). cSS pooled prevalence was 34% (95% confidence interval [CI] 26%-41%; I 2 87.94%; p < 0.001): focal cSS prevalence was 14% (95% CI 12%-16%; I 2 6.75%; p = 0.37), and disseminated cSS prevalence was 20% (95% CI 13%-26%; I 2 90.39%; p < 0.001). During a mean follow-up of 3.1 years (range 1-4 years), 162/1,239 patients experienced a symptomatic ICH-pooled incidence rate 6.9% per year (95% CI 3.9%-9.8% per year; I 2 83%; p < 0.001). ICH incidence rates per year according to cSS status were 3.9% (95% CI 1.7%-6.1%; I 2 70%; p = 0.018) for patients without cSS, 11.1% (95% CI 7%-15.2%; I 2 56.8%; p = 0.074) for cSS presence, 9.1% (95% CI 5.5%-12.8%; I 2 0%; p = 0.994) for focal cSS, and 12.5% (95% CI 5.3%-19.7%; I 2 73.2%; p = 0.011) for disseminated cSS. In adjusted pooled analysis, any cSS presence was independently associated with increased future ICH risk (adjHR 2.14; 95% CI 1.19-3.85; p < 0.0001). Focal cSS was linked with ICH risk (adjHR 2.11; 95% CI 1.31-2.41; p = 0.002), while disseminated cSS conferred the strongest bleeding risk (adjHR 4.28; 95% CI 2.91-6.30; p < 0.0001).
Conclusion: In patients with CAA, cSS presence and extent are the most important MRI prognostic risk factors for future ICH, likely useful in treatment planning.
Classification of evidence: This study provides Class III evidence that in symptomatic CAA survivors with baseline T2*-MRI, cSS (particularly if disseminated, i.e., affecting >3 sulci) increases the risk of future ICH.
© 2019 American Academy of Neurology.
Figures
References
-
- Charidimou A, Linn J, Vernooij MW, et al. . Cortical superficial siderosis: detection and clinical significance in cerebral amyloid angiopathy and related conditions. Brain 2015;138:2126–2139. - PubMed
-
- Linn J, Wollenweber FA, Lummel N, et al. . Superficial siderosis is a warning sign for future intracranial hemorrhage. J Neurol 2013;260:176–181. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials