

A nationwide causal mediation analysis of survival following ST-elevation myocardial infarction
- PMID: 31732655
- PMCID: PMC7229897
- DOI: 10.1136/heartjnl-2019-315760
A nationwide causal mediation analysis of survival following ST-elevation myocardial infarction
Abstract
Objective: International studies report a decline in mortality following ST-elevation myocardial infarction (STEMI). The extent to which the observed improvements in STEMI survival are explained by temporal changes in patient characteristics and utilisation of treatments is unknown.
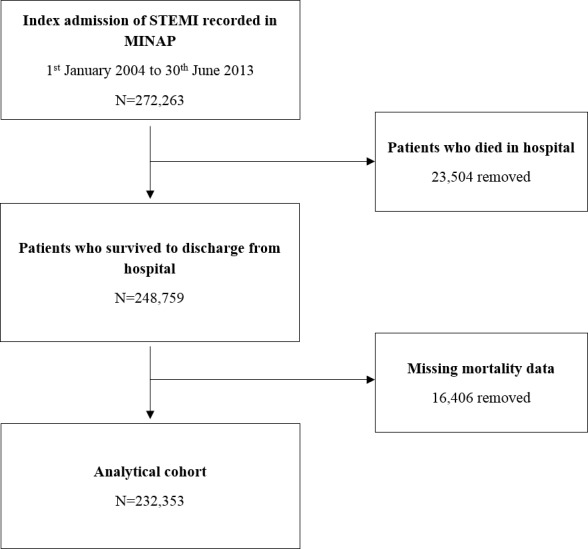
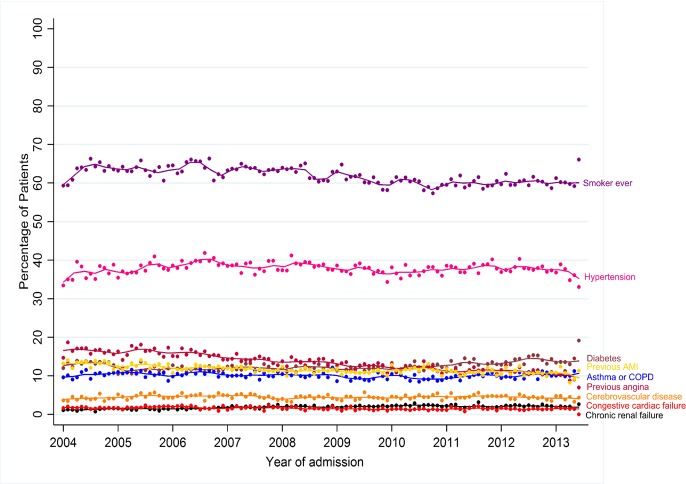
Methods: Cohort study using national registry data from the Myocardial Ischaemia National Audit Project between first January 2004 and 30th June 2013. 232 353 survivors of hospitalisation with STEMI as recorded in 247 hospitals in England and Wales. Flexible parametric survival modelling and causal mediation analysis were used to estimate the relative contribution of temporal changes in treatments and patient characteristics on improved STEMI survival.
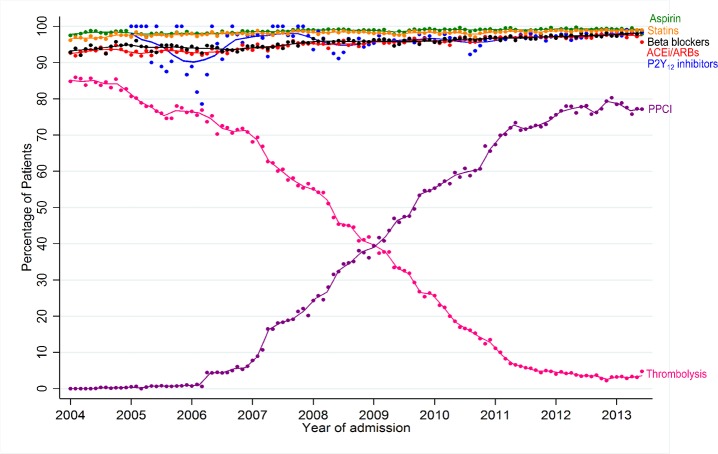
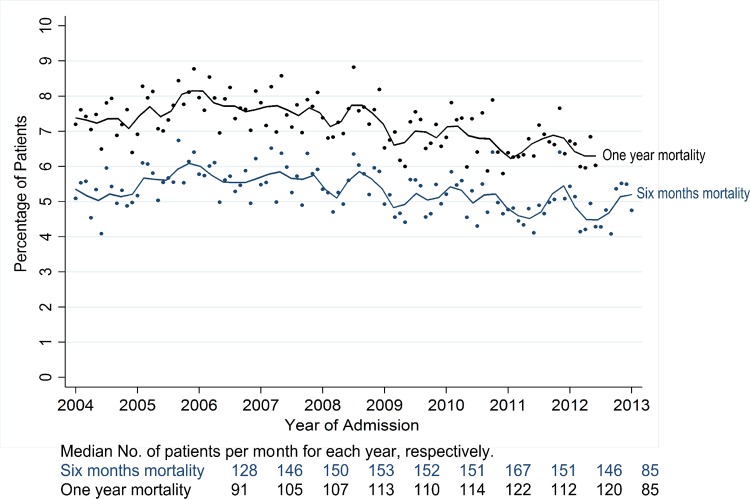
Results: Over the study period, unadjusted survival at 6 months and 1 year improved by 0.9% and 1.0% on average per year (HR: 0.991, 95% CI: 0.988 to 0.994 and HR: 0.990, 95% CI: 0.987 to 0.993, respectively). The uptake of primary percutaneous coronary intervention (PCI) (HR: 1.025, 95% CI: 1.021 to 1.028) and increased prescription of P2Y12 inhibitors (HR: 1.035, 95% CI: 1.031 to 1.039) were significantly associated with improvements in 1-year survival. Primary PCI explained 16.8% (95% CI: 10.8% to 31.6%) and 13.2% (9.2% to 21.9%) of the temporal survival improvements at 6 months and 1 year, respectively, whereas P2Y12 inhibitor prescription explained 5.3% (3.6% to 8.8%) of the temporal improvements at 6 months but not at 1 year.
Conclusions: For STEMI in England and Wales, improvements in survival between 2004 and 2013 were significantly explained by the uptake of primary PCI and increased use of P2Y12 inhibitors at 6 months and primary PCI only at 1 year.
Trial registration number: NCT03749694.
Keywords: acute coronary syndromes; acute myocardial infarction; electronic medical records; epidemiology; quality and outcomes of care.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: CPG reports personal fees and non-financial support from AstraZeneca, non-financial support from BMS-Pfizer, personal fees from Bayer, personal fees from Novartis, personal fees from Vifor Pharma, outside the submitted work. KAAF reports grants and personal fees from Bayer/Janssen, grants from AstraZeneca, personal fees from Sanofi/Regeneron, personal fees from Verseon, outside the submitted work.
Figures
References
-
- Szummer K, Wallentin L, Lindhagen L, et al. . Improved outcomes in patients with ST-elevation myocardial infarction during the last 20 years are related to implementation of evidence-based treatments: experiences from the SWEDEHEART registry 1995–2014. Eur Heart J 2017;38:3056–65. 10.1093/eurheartj/ehx515 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous