

'New Medicine Service': supporting adherence in people starting a new medication for a long-term condition: 26-week follow-up of a pragmatic randomised controlled trial
- PMID: 31732700
- PMCID: PMC7146933
- DOI: 10.1136/bmjqs-2018-009177
'New Medicine Service': supporting adherence in people starting a new medication for a long-term condition: 26-week follow-up of a pragmatic randomised controlled trial
Abstract
Objective: To examine the effectiveness and cost-effectiveness of the community pharmacy New Medicine Service (NMS) at 26 weeks.
Methods: Pragmatic patient-level parallel randomised controlled trial in 46 English community pharmacies. 504 participants aged ≥14, identified in the pharmacy when presenting a prescription for a new medicine for predefined long-term conditions, randomised to receive NMS (n=251) or normal practice (n=253) (NMS intervention: 2 consultations 1 and 2 weeks after prescription presentation). Adherence assessed through patient self-report at 26-week follow-up. Intention-to-treat analysis employed. National Health Service (NHS) costs calculated. Disease-specific Markov models estimating impact of non-adherence combined with clinical trial data to calculate costs per extra quality-adjusted life-year (QALY; NHS England perspective).
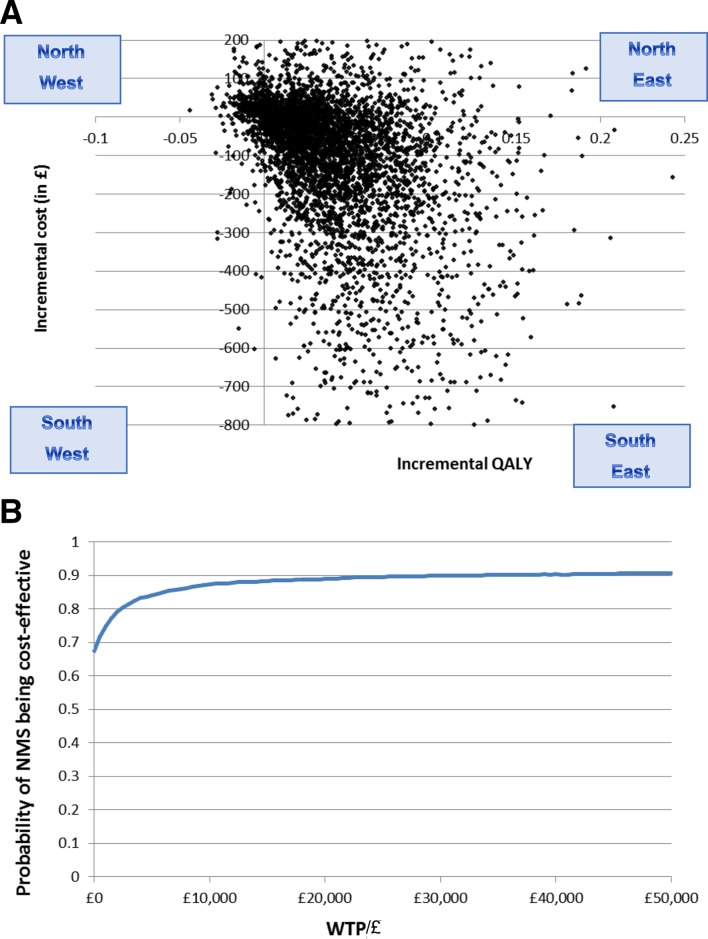
Results: Unadjusted analysis: of 327 patients still taking the initial medicine, 97/170 (57.1%) and 103/157 (65.6%) (p=0.113) patients were adherent in normal practice and NMS arms, respectively. Adjusted intention-to-treat analysis: adherence OR 1.50 (95% CI 0.93 to 2.44, p=0.095), in favour of NMS. There was a non-significant reduction in 26-week NHS costs for NMS: -£104 (95% CI -£37 to £257, p=0.168) per patient. NMS generated a mean of 0.04 (95% CI -0.01 to 0.13) more QALYs per patient, with mean reduction in lifetime cost of -£113.9 (-1159.4, 683.7). The incremental cost-effectiveness ratio was -£2758/QALY (2.5% and 97.5%: -38 739.5, 34 024.2. NMS has an 89% probability of cost-effectiveness at a willingness to pay of £20 000 per QALY.
Conclusions: At 26-week follow-up, NMS was unable to demonstrate a statistically significant increase in adherence or reduction in NHS costs, which may be attributable to patient attrition from the study. Long-term economic evaluation suggested NMS may deliver better patient outcomes and reduced overall healthcare costs than normal practice, but uncertainty around this finding is high.
Trial registration number: NCT01635361, ISRCTN23560818, ISRCTN23560818, UKCRN12494.
Keywords: compliance; cost-effectiveness; decision analysis; pharmacists; randomised controlled trial.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Medication non-adherence: an overlooked target for quality improvement interventions.BMJ Qual Saf. 2020 Apr;29(4):271-273. doi: 10.1136/bmjqs-2019-009984. Epub 2019 Dec 20. BMJ Qual Saf. 2020. PMID: 31862775 No abstract available.
References
-
- Department of Health Pharmacy in England: Building on strengths - delivering the future, 2008. Available: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicati...
-
- Leventhal H, Cameron L. Behavioral theories and the problem of compliance. Patient Educ Couns 1987;10:117–38. 10.1016/0738-3991(87)90093-0 - DOI
-
- Elliott RA, Clifford S, Barber N, et al. . The cost effectiveness of a pharmacy Advisory service to improve adherence to medicines. Pharmacy World and Science 2008;30:17–23. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical