

Resolution in bullous pemphigoid
- PMID: 31732776
- PMCID: PMC6881416
- DOI: 10.1007/s00281-019-00759-y
Resolution in bullous pemphigoid
Abstract
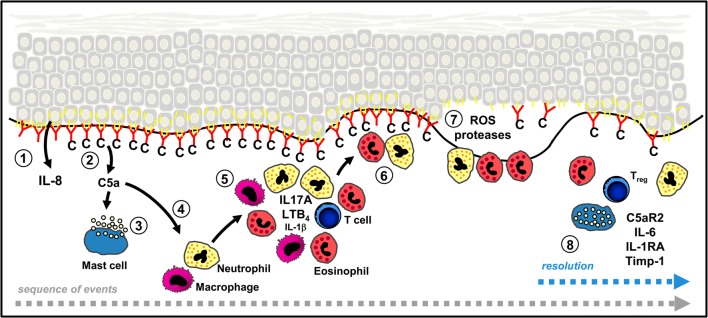
Pemphigoid diseases are a group of autoimmune blistering skin diseases defined by an immune response against certain components of the dermal-epidermal adhesion complex. They are prototypical, autoantibody-driven, organ-specific diseases with the emergence of inflammatory skin lesions dependent on the recruitment of immune cells, particularly granulocytes, into the skin. During an acute flare of disease, inflammatory skin lesions typically progressing from erythema through urticarial plaques to subepidermal blisters erosions erupt and, finally, completely resolve, thus illustrating that resolution of inflammation is continuously executed in pemphigoid disease patients and can be directly monitored on the skin. Despite these superb conditions for examining resolution in pemphigoid diseases as paradigm diseases for antibody-induced tissue inflammation, the mechanisms of resolution in pemphigoid are underinvestigated and still largely elusive. In the last decade, mouse models for pemphigoid diseases were developed, which have been instrumental to identify several key pathways for the initiation of inflammation in these diseases. More recently, also protective pathways, specifically IL-10 and C5aR2 signalling on the molecular level and Tregs on the cellular level, counteracting skin inflammation have been highlighted and may contribute to the continuous execution of resolution in pemphigoid diseases. The upstream orchestrators of this process are currently under investigation. Pemphigoid disease patients, particularly bullous pemphigoid patients, who are predominantly above 75 years of age, often succumb to the side effects of the immunosuppressive therapeutics nowadays still required to suppress the disease. Pemphigoid disease patients may therefore represent a group of patients benefiting most substantially from the introduction of non-immunosuppressive, proresolving therapeutics into the treatment regimens for their disease.
Keywords: Autoimmunity; Blistering; Bullous pemphigoid; Complement; IL-17; Pathophysiology; Resolution.
Figures

References
-
- Amber KT, Murrell DF, Schmidt E, Joly P, Borradori L. Autoimmune subepidermal bullous diseases of the skin and mucosae: clinical features, diagnosis, and management. Clin Rev Allergy Immunol. 2018;54(1):26–51. - PubMed
-
- Schmidt E, Groves R. Immunobullous diseases. In: Griffith C, Barker J, Chalmers BT, Creamer D, editors. Rook’s textbook of dermatology, part 3, chapter 50. 9. Chichester: Wiley-Blackwell; 2016. pp. 1–56.
-
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381(9863):320–332. - PubMed
-
- Hubner F, Recke A, Zillikens D, Linder R, Schmidt E. Prevalence and age distribution of pemphigus and pemphigoid diseases in Germany. J Invest Dermatol. 2016;136(12):2495–2498. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
