

Macrophage Activation Syndrome and Secondary Hemophagocytic Lymphohistiocytosis in Childhood Inflammatory Disorders: Diagnosis and Management
- PMID: 31732958
- PMCID: PMC7334831
- DOI: 10.1007/s40272-019-00367-1
Macrophage Activation Syndrome and Secondary Hemophagocytic Lymphohistiocytosis in Childhood Inflammatory Disorders: Diagnosis and Management
Abstract
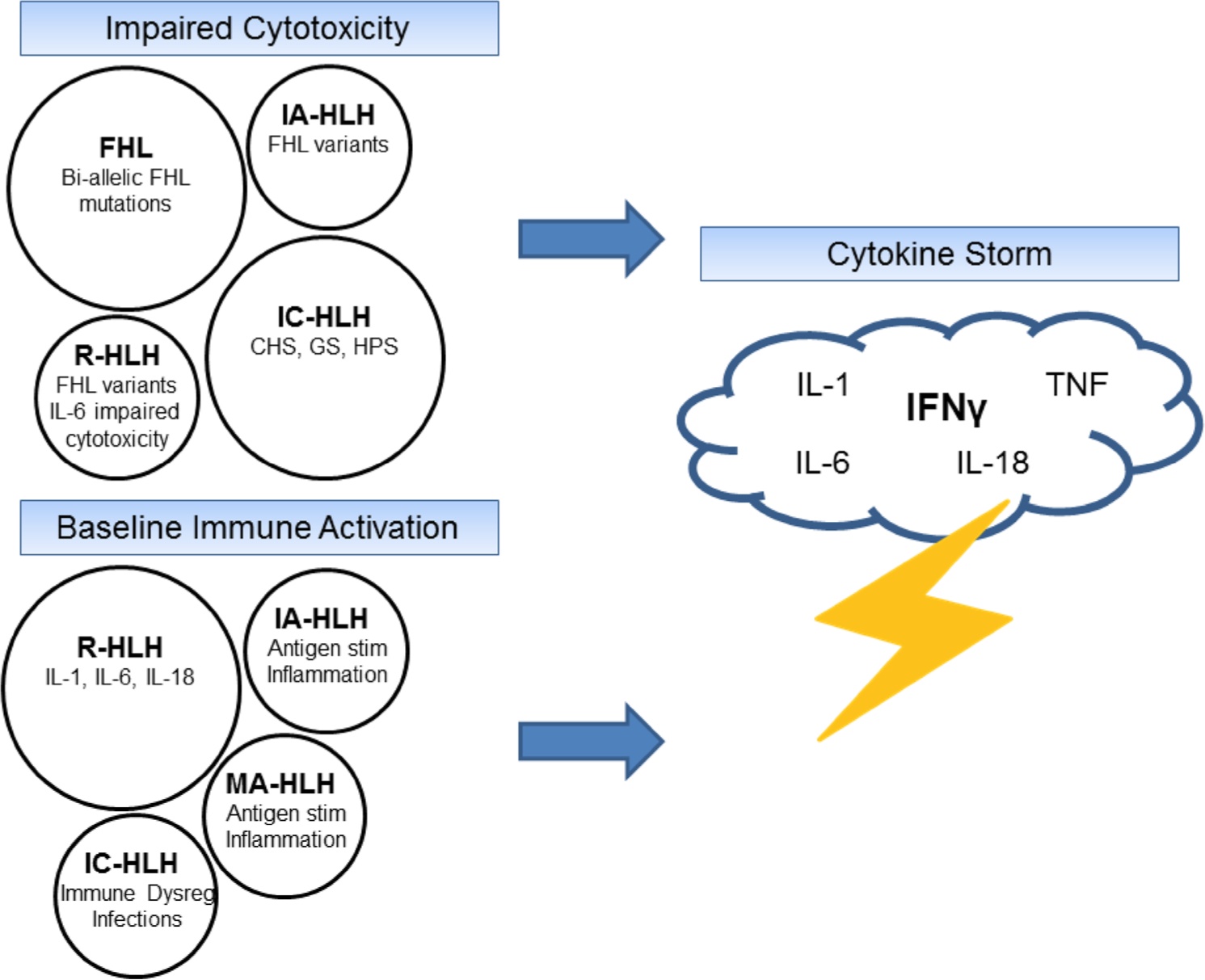
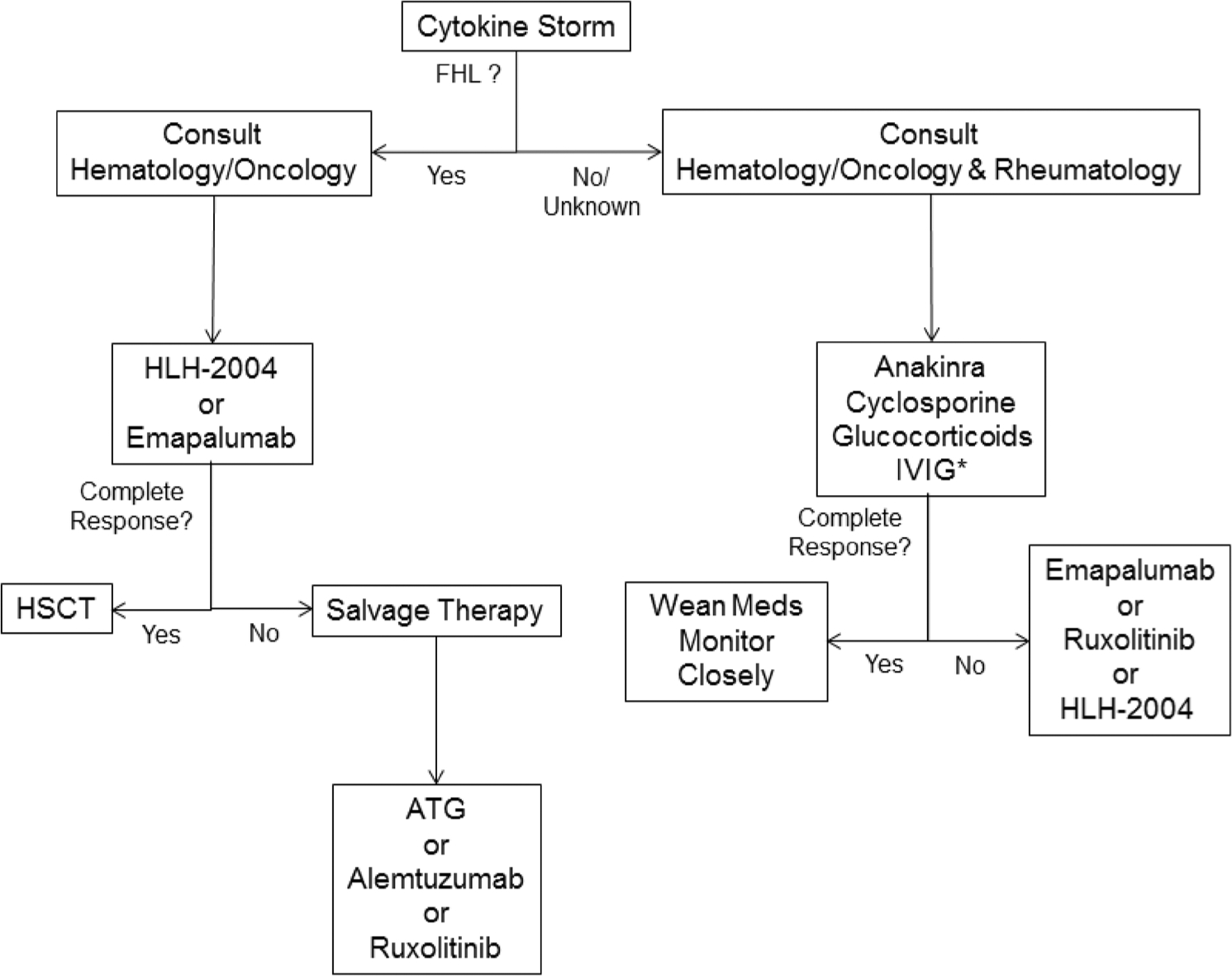
Macrophage activation syndrome (MAS), a form of secondary hemophagocytic lymphohistiocytosis, is a frequently fatal complication of a variety of pediatric inflammatory disorders. MAS has been most commonly associated with systemic juvenile idiopathic arthritis (sJIA), as approximately 10% of children with sJIA develop fulminant MAS, with another 30-40% exhibiting a more subclinical form of the disease. Children with other rheumatologic conditions such as systemic lupus erythematosus and Kawasaki disease are also at risk for MAS. Moreover, MAS also complicates various genetic autoinflammatory disorders such as gain of function mutations in the cytosolic inflammasome NLRC4, pediatric hematologic malignancies (e.g., T-cell lymphoma), and primary immunodeficiencies characterized by immune dysregulation. Disease-specific and broadly inclusive diagnostic criteria have been developed to facilitate the diagnosis of MAS. Recently, simple screening tools such as the serum ferritin to erythrocyte sedimentation rate ratio have been proposed. Early diagnosis and rapid initiation of immunosuppression are essential for the effective management of MAS. With a better understanding of the pathophysiology of MAS and the advent of novel therapeutics, a broad immunosuppressive approach to treatment is giving way to targeted anti-cytokine therapies. These treatments include agents that block interleukin-1 (IL-1), IL-6, IL-18, interferon-γ, as well as inhibitors of downstream targets of cytokine signaling (e.g., Janus kinases). Increased early recognition of MAS among pediatric inflammatory disorders combined with the use of effective and less toxic cytokine-targeted therapies should lower the mortality of this frequently fatal disorder.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
